Wed, Apr 24, 2024
Volume 1, Issue 3 (12-2015)
Iran J Neurosurg 2015, 1(3): 26-29 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Tine I, A. Diop A, Mbengue A, K. Wimenga A, S. Mudekereza P, B. Badiane S. A Rare Cause of Obstructive Chronic Hydrocephalus in an Adult Patient: A Case Report of Fourth Ventricle's Foramina Idiopathic Stenosis. Iran J Neurosurg 2015; 1 (3) :26-29
URL: http://irjns.org/article-1-21-en.html
URL: http://irjns.org/article-1-21-en.html
Ibrahima Tine * 

 1, Abdou A. Diop1 , Ababacar Mbengue2 , Abdou K. Wimenga3 , Paterne S. Mudekereza3 , Seydou B. Badiane3
1, Abdou A. Diop1 , Ababacar Mbengue2 , Abdou K. Wimenga3 , Paterne S. Mudekereza3 , Seydou B. Badiane3
1, Abdou A. Diop1 , Ababacar Mbengue2 , Abdou K. Wimenga3 , Paterne S. Mudekereza3 , Seydou B. Badiane3
1- Unit of Neurosurgery, Principal Hospital of Dakar, Dakar, Senegal, West Africa
2- Department of Imaging, Principal Hospital of Dakar, Dakar, Senegal, West Africa
3- Department of Neurosurgery, University Hospital Center of Fann, Dakar, Senegal, West Africa
2- Department of Imaging, Principal Hospital of Dakar, Dakar, Senegal, West Africa
3- Department of Neurosurgery, University Hospital Center of Fann, Dakar, Senegal, West Africa
Full Text [PDF 440 kb]
(3782 Downloads)
| Abstract (HTML) (5658 Views)
is often linked to an inflammatory process secondary to infection or hemorrhage. In rare cases, no cause is identified (2,4,5). According to Carpentier et al. (1), three different types of obstruction of the foramina of Luschka can occur. In the dysgenesis of the foramen of Luschka, openings in the membrane would lead to a valvular mechanism with intermittent flow of CSF. In the agenesis of the foramen of Luschka, punctiform openings in the membrane would slow the flow of CSF from the ventricular system. In the third type, an arachnoiditis would occur in response to an inflammatory process. There are no typical clinical characteristics. Mainly, signs of compensated intracranial hypertension were reported as headache, nausea and vomiting, papillary edema. Gait ataxia and vertigo were reported as in our case. But acute hydrocephalus with an altered state of consciousness can occur spontaneously or by a minimal head injury (7,8). The diagnosis of hydrocephalus due to fourth ventricle’s outlet obstruction can be suspected in case of an imaging study (CT scan or MRI) that shows dilation of all 4 ventricles but mainly involving the forth, and a patent cerebral aqueduct (3,4,8). A significant increase of the lateral recesses with bulging into the cerebellopontine angle may suggest obstruction of the lateral foramina. In Cine-MRI imaging, the CSF flow dynamic can be studied, and help to precisely determine the level of stenosis (8). The absence of cerebrospinal fluid flow from the median outlet may suggest the diagnosis but the CSF flow analysis by MR sequences is less effective at this location than at the cerebral
Full Text: (1516 Views)
Introduction
Idiopathic stenosis of the foramina of Magendie and Luschka is a rare but well-established cause of obstructive hydrocephalus involving the fourth ventricle (5). In children, it is usually the consequence of posterior cerebral fossa (PCF) malformations and in adults, the occlusion is rather acquired than congenital, often linked to an inflammatory process, or sometimes to an infection, head trauma, intraventricular hemorrhage, tumors or Arnold–Chiari malformation (7). It can be treated with a CSF shunt or a suboccipital craniotomy and opening of the membrane obstructing the foramen of Magendie. As neuroendoscopic procedures improved, endoscopic third ventriculostomy (ETV) becomes an excellent option for treatment of these patients because of its efficiency and lower risk than other procedures (3, 6). Here we report a case of idiopathic stenosis of the foramina of Magendie and Luschka in an adult patient successfully treated by ETV.
Case Presentation
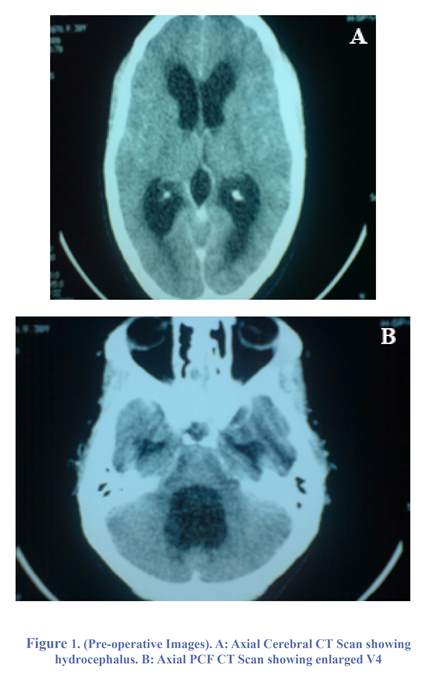
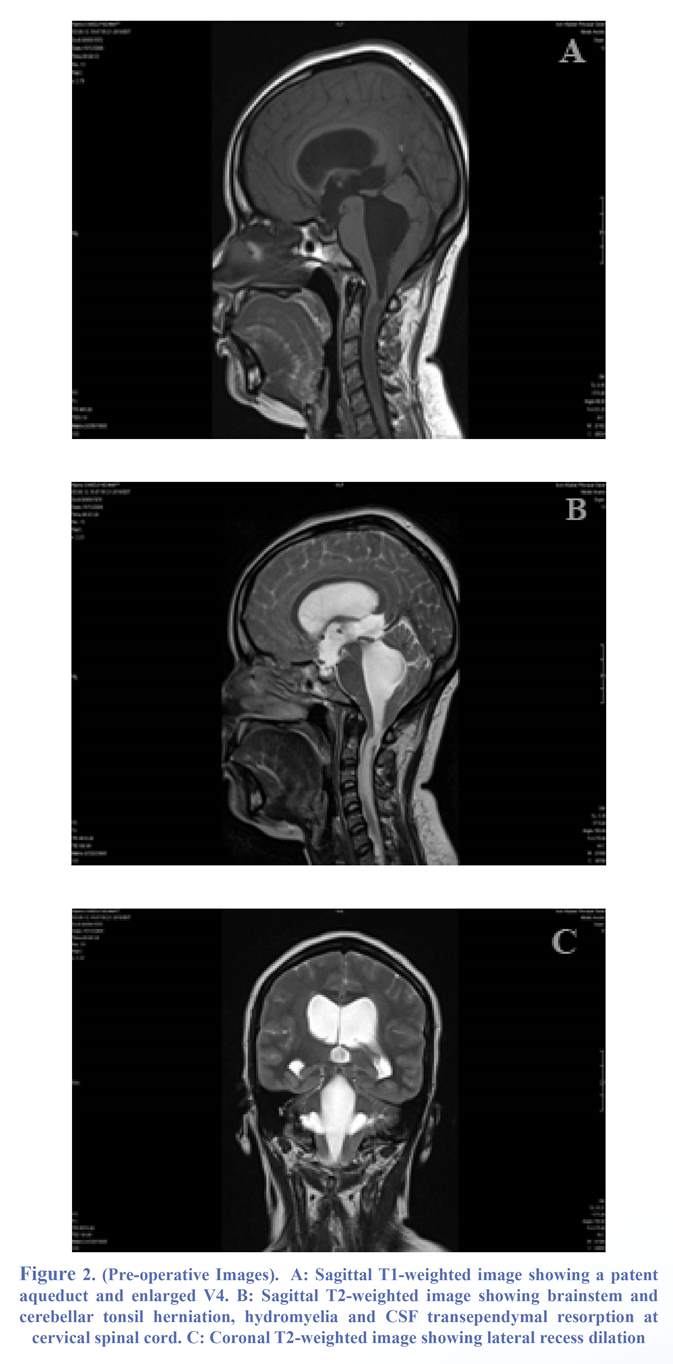
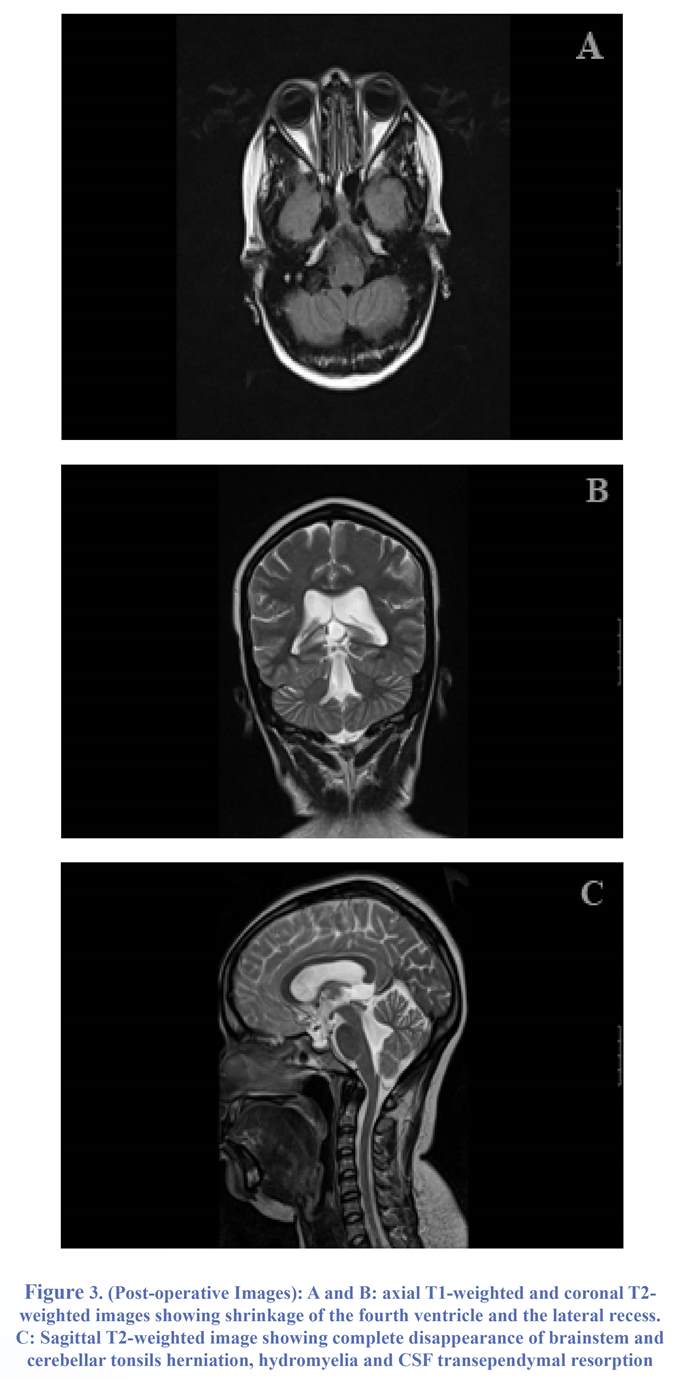
We reported the case of a 40-year-old woman with no particular medical history who developed high cranial pressure symptoms like headaches, nausea, photophobia and vertigo for several months and more recently gait disturbance. There was no history of infection or head injury. Physical examination was normal except for gait ataxia. A first CT scan showed quadri-ventricular hydrocephalus involving mainly the fourth ventricle with dilated lateral recesses (Figure 1). Then a craniocervical MRI was prescribed for more accuracy and confirmed hydrocephalus and also tonsils and brainstem (fourth ventricle) herniation through the foramen magnum. Hydromyelia and transependymal resorption of cerebrospinal fluid (CSF) were shown as a hyperintense signal on T2 weighted MRI of cervical spinal cord (Figure 2). Biological analyses results were normal. She underwent ETV. No complication was observed. The patient became asymptomatic during the weeks following the surgical procedure and remained stable at a mean follow-up interval of 20 months. Postoperative MR images demonstrated regression of the hydrocephalus and complete disappearance of brainstem and cerebellar tonsil herniation, hydromylia and the hyperintense signal on T2 weighted MRI of cervical spinal cord (Figure 3).
Discussion
Obstruction of the fourth ventricle’s exits is a common cause of hydrocephalus. It is usually congenital in children with PCF malformation like Dandy-Walker, Chiari malformation, tuberous sclerosis, spina bifida, platybasia, achondroplasia, basilar impression and atlanto-occipital fusion; but in adults it
Idiopathic stenosis of the foramina of Magendie and Luschka is a rare but well-established cause of obstructive hydrocephalus involving the fourth ventricle (5). In children, it is usually the consequence of posterior cerebral fossa (PCF) malformations and in adults, the occlusion is rather acquired than congenital, often linked to an inflammatory process, or sometimes to an infection, head trauma, intraventricular hemorrhage, tumors or Arnold–Chiari malformation (7). It can be treated with a CSF shunt or a suboccipital craniotomy and opening of the membrane obstructing the foramen of Magendie. As neuroendoscopic procedures improved, endoscopic third ventriculostomy (ETV) becomes an excellent option for treatment of these patients because of its efficiency and lower risk than other procedures (3, 6). Here we report a case of idiopathic stenosis of the foramina of Magendie and Luschka in an adult patient successfully treated by ETV.
Case Presentation
We reported the case of a 40-year-old woman with no particular medical history who developed high cranial pressure symptoms like headaches, nausea, photophobia and vertigo for several months and more recently gait disturbance. There was no history of infection or head injury. Physical examination was normal except for gait ataxia. A first CT scan showed quadri-ventricular hydrocephalus involving mainly the fourth ventricle with dilated lateral recesses (Figure 1). Then a craniocervical MRI was prescribed for more accuracy and confirmed hydrocephalus and also tonsils and brainstem (fourth ventricle) herniation through the foramen magnum. Hydromyelia and transependymal resorption of cerebrospinal fluid (CSF) were shown as a hyperintense signal on T2 weighted MRI of cervical spinal cord (Figure 2). Biological analyses results were normal. She underwent ETV. No complication was observed. The patient became asymptomatic during the weeks following the surgical procedure and remained stable at a mean follow-up interval of 20 months. Postoperative MR images demonstrated regression of the hydrocephalus and complete disappearance of brainstem and cerebellar tonsil herniation, hydromylia and the hyperintense signal on T2 weighted MRI of cervical spinal cord (Figure 3).
Discussion
Obstruction of the fourth ventricle’s exits is a common cause of hydrocephalus. It is usually congenital in children with PCF malformation like Dandy-Walker, Chiari malformation, tuberous sclerosis, spina bifida, platybasia, achondroplasia, basilar impression and atlanto-occipital fusion; but in adults it
is often linked to an inflammatory process secondary to infection or hemorrhage. In rare cases, no cause is identified (2,4,5). According to Carpentier et al. (1), three different types of obstruction of the foramina of Luschka can occur. In the dysgenesis of the foramen of Luschka, openings in the membrane would lead to a valvular mechanism with intermittent flow of CSF. In the agenesis of the foramen of Luschka, punctiform openings in the membrane would slow the flow of CSF from the ventricular system. In the third type, an arachnoiditis would occur in response to an inflammatory process. There are no typical clinical characteristics. Mainly, signs of compensated intracranial hypertension were reported as headache, nausea and vomiting, papillary edema. Gait ataxia and vertigo were reported as in our case. But acute hydrocephalus with an altered state of consciousness can occur spontaneously or by a minimal head injury (7,8). The diagnosis of hydrocephalus due to fourth ventricle’s outlet obstruction can be suspected in case of an imaging study (CT scan or MRI) that shows dilation of all 4 ventricles but mainly involving the forth, and a patent cerebral aqueduct (3,4,8). A significant increase of the lateral recesses with bulging into the cerebellopontine angle may suggest obstruction of the lateral foramina. In Cine-MRI imaging, the CSF flow dynamic can be studied, and help to precisely determine the level of stenosis (8). The absence of cerebrospinal fluid flow from the median outlet may suggest the diagnosis but the CSF flow analysis by MR sequences is less effective at this location than at the cerebral
aqueduct. High resolution MRI may directly visualize the membrane involving the occlusion of the foramen of Magendie as previously reported in a child. However, the membrane was actually visible only on the sagittal T1-weighted MR images (8). On T2-weighted MR images, the membrane was not so evident. Ventriculography was used but it is an invasive method. In our case, MRI also indicated cerebellar tonsils and fourth ventricle herniation through the foramen magnum with normal PCF. Dilation of ependymal central channel with transependymal resorption of CSF mimicking low grade glioma was also noted at the cervical level of spinal cord in our case. This is secondary to the high pressure noted in the fourth ventricle. For the treatment of hydrocephalus due to fourth ventricle’s outlet
artery toward the floor of the third ventricle. These distortions may prevent a safe ETV procedure. Minimal dilation of the supratentorial ventricular system can also make ETV procedure difficult (3). Longatti et al. (6) proposed the opening of the foramen of Magendie by transaqueductal endoscopic navigation in fourth ventricle using a flexible endoscope. This technique is not easy and present higher risk of encephalic injury than ETV. Recently, Gianetti et al. (3) proposed a new technique using direct endoscopic approach of the fourth ventricle through a paramedian subocciptal burr hole. This technique can be an alternative for ETV for treatment of hydrocephalus due to obstruction of fourth ventricle’s outlets. Idiopathic obstruction of fourth ventricle’s foramina is rare. Its diagnosis is facilitated by MRI study. ETV is the safest treatment although there are other effective methods.
Funding
None.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
Funding
None.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- Carpentier A, Brunelle F, Philippon J, Clemenceau S: Obstruction of Magendie’s and Luschka’s foramina. Cine-MRI, aetiology and pathogenesis. Acta Neurochir. 2001; 143:517–522.
- Fuentes S, Métellus P, Adetchessi T, Dufour H, Grisoli F. [Idiopathic acute obstructive hydrocephalus. Case report]. Neurochirurgie. 2006 Feb;52(1):47-51. ( article in French)
- Giannetti AV, Malheiros JA, da Silva MC. Fourth ventriculostomy: an alternative treatment for hydrocephalus due to atresia of the Magendie and Luschka foramina. J Neurosurg Pediatr. 2011 Feb;7(2):152-6.
- Hashish H, Guenot M, Mertens P, Sindou M: [Chronic hydrocephalus in an adult due to congenital membranous occlusion of the apertura mediana ventriculi quartii (foramen of Magendie). Report of two cases and review of the literature.] Neurochirurgie 1999; 45:232–236. (article in French)
- Karachi C, Le Guérinel C, Brugières P, Melon E, Decq P. Hydrocephalus due to idiopathic stenosis of the foramina of Magendie and Luschka. Report of three cases. J Neurosurg. 2003 Apr;98(4):897-902.
- Longatti P, Fiorindi A, Feletti A, Baratto V: Endoscopic opening of the foramen of magendie using transaqueductal navigation for membrane obstruction of the fourth ventricle outlets. Technical note. J Neurosurg. 2006; 105:924-927.
- Mohanty A, Anandh B, Kolluri VR, Praharaj SS: Neuroendoscopic third ventriculostomy in the management of fourth ventricular outlet obstruction. Minim Invasive Neurosurg. 1999; 42:18-21.
- Rougier A, Ménégon P. MRI evidence of membranous occlusion of the foramen of Magendie Acta Neurochir. 2009; 151:693–694.
Type of Study: Case report |
Subject:
Gamma Knife Radiosurgery
References
1. Carpentier A, Brunelle F, Philippon J, Clemenceau S: Obstruction of Magendie's and Luschka's foramina. Cine-MRI, aetiology and pathogenesis. Acta Neurochir. 2001; 143:517–522. [DOI:10.1007/s007010170083] [PMID]
2. Fuentes S, Métellus P, Adetchessi T, Dufour H, Grisoli F. [Idiopathic acute obstructive hydrocephalus. Case report]. Neurochirurgie. 2006 Feb;52(1):47-51. (article in French) [DOI:10.1016/S0028-3770(06)71169-9]
3. Giannetti AV, Malheiros JA, da Silva MC. Fourth ventriculostomy: an alternative treatment for hydrocephalus due to atresia of the Magendie and Luschka foramina. J Neurosurg Pediatr. 2011 Feb;7(2):152-6. [DOI:10.3171/2010.11.PEDS1080] [PMID]
4. Hashish H, Guenot M, Mertens P, Sindou M: [Chronic hydrocephalus in an adult due to congenital membranous occlusion of the apertura mediana ventriculi quartii (foramen of Magendie). Report of two cases and review of the literature.] Neurochirurgie 1999; 45:232–236. (article in French) [PMID]
5. Karachi C, Le Guérinel C, Brugières P, Melon E, Decq P. Hydrocephalus due to idiopathic stenosis of the foramina of Magendie and Luschka. Report of three cases. J Neurosurg. 2003 Apr;98(4):897-902. [DOI:10.3171/jns.2003.98.4.0897] [PMID]
6. Longatti P, Fiorindi A, Feletti A, Baratto V: Endoscopic opening of the foramen of magendie using transaqueductal navigation for membrane obstruction of the fourth ventricle outlets. Technical note. J Neurosurg. 2006; 105:924-927. [DOI:10.3171/jns.2006.105.6.924] [PMID]
7. Mohanty A, Anandh B, Kolluri VR, Praharaj SS: Neuroendoscopic third ventriculostomy in the management of fourth ventricular outlet obstruction. Minim Invasive Neurosurg. 1999; 42:18-21. [DOI:10.1055/s-2008-1053362] [PMID]
8. Rougier A, Ménégon P. MRI evidence of membranous occlusion of the foramen of Magendie Acta Neurochir. 2009; 151:693–694.
| Rights and Permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information:
IrJNS Office, Guilan Road Trauma Research Center, Poursina Hospital, Namjoo St, Rasht, Guilan, Iran.
Publisher Tel : +9821 45355555 , 45355000
Email: ir.journalofneurosurgery@gmail.com, info@irjns.org
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information:
IrJNS Office, Guilan Road Trauma Research Center, Poursina Hospital, Namjoo St, Rasht, Guilan, Iran.
Publisher Tel : +9821 45355555 , 45355000
Email: ir.journalofneurosurgery@gmail.com, info@irjns.org
