


BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://irjns.org/article-1-78-en.html

 , Ali Babaei Jandaghi1 , Ehsan Kazemnejad-Leili2 , Leila Kouchakinejad-Eramsadati2 , Marieh Hosseinpour * 3
, Ali Babaei Jandaghi1 , Ehsan Kazemnejad-Leili2 , Leila Kouchakinejad-Eramsadati2 , Marieh Hosseinpour * 3
2- Guilan Road Trauma Research Center, Department of Neurosurgery, Poursina Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran
3- Neuroscience Research Center, Department of Neurosurgery, Poursina Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran , bak-sou@hotmail.com
Subdural Hygroma in Head Trauma Patients Admitted to a Hospital in Northern Iran
Shahrokh Yousefzadeh-Chabok 1,2, Ali Babaei Jandaghi 1,2, Ehsan Kazemnejad-Leili 2, Leila Kouchakinejad-Eramsadati 2, Marieh Hosseinpour 1*
1 Neuroscience Research Center, Department of Neurosurgery, Poursina Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran
2 Guilan Road Trauma Research Center, Department of Neurosurgery, Poursina Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran
* Corresponding Author Address: Neuroscience Research Center, Department of Neurosurgery, Poursina Hospital, Namjoo Street, Rasht, Iran. Tel: +981333311473. Fax: +981333311473. Email: bak-sou@hotmail.com
Article Type: Research Article Received: October 8, 2016, Last Revised: March 1, 2017, Accepted: March 2, 2017, Published: March 31, 2017
Abstract
Background & Aim: Post-traumatic subdural hygroma can be associated with subdural or epidural hematoma. It is usually silent with mild symptoms and often disappears spontaneously needing no treatment. In this study, we investigated the clinical characteristics of subdural hygroma in patients with traumatic brain injury.
Methods and Materials/Patients: In a cross-sectional study, data of 3244 patients with head injury admitted to Poursina hospital were collected through a questionnaire which included variables of age, sex, GCS on admission, mechanism of trauma, accompanying cranial injuries and treatments, unilateral/bilateral hygroma, and size, volume, and location of hygroma. Finally, the data were analyzed using SPSS (version 19) and descriptive statistics.
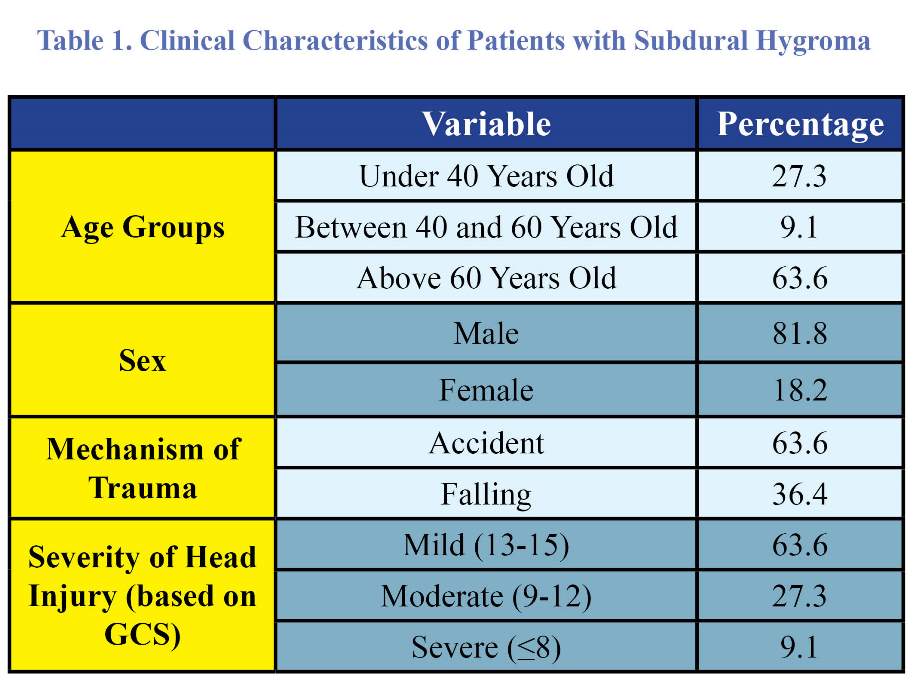
Results: In this study, 81.8% of patients were men and 18.2% women with mean age of 60.91±26.07 years old. Accident was the most common cause (63.6%) and the severity of head injury was mild in majority of patients (63.6%) according to GCS. The average time of diagnosis was 10.4 days after the head injury was located in frontal (36.4%) and fronto-parietal (36.4%) areas in most patients. Most of the accompanying cranial injuries were brain contusion (36.4%) and subarachnoid hemorrhage (27.3%). The majority of patients (81.8%) underwent conservative treatment and showed a favorable outcome (63.6%).
Conclusion: Most of the times, subdural hygroma is observed in older people and disappears over time with vanishing clinical symptoms. Most cases have to undergo conservative treatment.
Keywords: Subdural Hygroma; Head Injury; Conservative Treatment
Please cite this paper as: Yousefzadeh-Chabok Sh, Babaei Jandaghi A, Kazemnejad-Leili E, Kouchakinejad-Eramsadati L, Hosseinpour M. Subdural Hygroma in Head Trauma Patients Admitted to a Hospital in Northern Iran. IrJNS. 2017;2(4):15-17
Introduction
Traumatic brain injury (TBI) is accounted as a major public health problem in the world. Severe head trauma can cause closed or open injuries, skull fractures, epidural, subdural hematoma or intracranial hemorrhage or less severe injuries such as posttraumatic hygromas [1]. Subdural accumulation of cerebrospinal fluid (CSF) after trauma is known as traumatic subdural hygroma also called traumatic subdural effusion (TSE) and external hydrocephalus (EHP) [2]. This is a common lesion of traumatic brain injury observed in 6% to 21.6% of patients [3]. Based on previous studies, the basic requirement for formation of subdural hygroma (SDG) is the subdural space for fluid accumulation; this space does not exist in normal condition but a mild trauma can separate the dura-arachnoid interface [4,5]. SDG has an interface layer composed of an arachnoid barrier layer and dura border cell layer [6]. It is a delayed lesion of head trauma, often silent and asymptomatic which disappears gradually, so in most cases this neurological lesion is undetected or neglected [1]. After detection of SDG, conservative treatment is usually the first choice aimed at reducing the symptoms of disease in patients. In extended hygromas, when there is mass effect and compressed brain tissue, surgery will be the effective remedy [1]. Although patients' improvement is good, some report that 28% of patients die, which is directly related to severity of primary head trauma [1]. Investigating this complication is, therefore, of high importance in head trauma patients. Despite of doing abundant research so far, many ambiguities remain about SDG which triggered us to examine this issue in patients with head trauma in Poursina Hospital, Rasht.
Methods and Materials/Patients
This cross-sectional study was conducted on 3244 patients with head trauma admitted to Poursina Hospital in Rasht (northern Iran). All of the participants signed informed written consent before participation. This study has been approved by the institutional review board of Guilan University of Medical Sciences. Primary information of patients such as age, sex, GCS on admission and trauma mechanism were collected. Serial CT scan was performed on admission, on second to seventh day (first week) and on eighth to fourteenth day (second week). Information of detected hygromas including size, extent, hygroma formation site, bilateral/unilateral (left or right) area and previous/on-admission as well as recent skull injuries and contusions, subarachnoid hemorrhage, subdural hematoma, epidural hematoma, and other data were recorded. Treatments were studied and applied. Data were analyzed using SPSS (version 19) and descriptive statistics.
Results
Of 3244 patients with brain injury, 11 (0.03%) had SDG, that nine (81.8%) and two (18.2%) of them were men and women, respectively, with mean age of 60.91±26.07 years, ranging from 22-91 years.
The main causes of SDG were accident (63.6%) and falling (36.4%). Consciousness level of patients were evaluated based on GCS on admission. So, severity of head injury was mild in seven patients (63.3%) (GCS=13-15), moderate in three patients (27.3%) and severe in one patient (9.1%) (GCS=3-8). Mean GCS was 12.91±2.34 in all of them (Table 1). Average time of diagnosis on CT scan was 10.4 days after trauma which appeared within the first week in most patients (81.8%). Hygroma was formed in four cases (36.4%) in the frontal, one case (9.1%) in the frontotemporal, four cases (36.4%) in fronto-parietal, one case (9.1%) in fronto-temporo-parietal and one case (9.1%) in temporal area of SDG space.
Table 1. Clinical Characteristics of Patients with Subdural Hygroma
Bilateral and unilateral SDGs were observed in eight (72.7%) and three patients (27.3%) (two patienys with left and one patient with right SDG), respectively. Most patients were reported as bilateral frontal and fronto-parietal SDG (Figure 1). The average thickness of SDG in patients was found to be 11.04 ±5.2 mm. The average volume of SDG was 29.45±32.38 ml. Most associated cranial injuries in CT images were brain contusion in four cases (36.4%) and subarachnoid hemorrhage (SAH) in three cases (27.3%). Other injuries observed included subdural hematoma (SDH) in two cases (18.2%), intracranial hemorrhage (ICH) in two cases (18.2%), epidural hematoma (EDH) in two patients (18.2%) and intraventricular hemorrhage (IVH) in one (9.1%) patient. Conservative treatment was applied on nine (81.8%) patients and only two cases (18.2%) were operated. The outcome of patients with SDG was assessed based on Glasgow Outcome Scale (GOS). Patients with good recovery and mild to moderate disability were classified in favorable outcome group, and patients having severe disability and vegetative state or who had died were classified in unfavorable outcome group. Accordingly, seven (63.6%) and four (36.7%) patients had favorable and unfavorable outcome, respectively.
Discussion
SDG is the accumulation of CSF, usually with modified compounds in subdural space [4,5,7] which can be the result of infection or any cranial surgery but trauma is the most common cause [5]. In this study, most patients with SDG (63.6%) were old (≥60 years). Considering the results of various studies, SDG is mostly observed in the elderly [8-11]. This is because most elderly people have varying degrees of brain atrophy [15] which can create subdural space. Consequently, CFS is accumulated in this space and forms SDG [5]. Most of our patients were men. Other studies showed similar results [4,11,12]. In this study, accident was the leading cause similar to Zaninin et al. study on patients with traumatic SDG [13]. Lee et al. also reported accident as the most common mechanism of trauma [4]. In this study, consciousness level of patients on admission was evaluated based on GCS. The mean GCS on admission was 12.2 in our study. In a study by Yousefzadeh-Chabok et al., GCS was 11.1 and in Park's study, it was reported as 14.1 after primary head injury. We found mean time of hygroma formation to be 10.4 days. In Zaninin et al. Study, it was reported as 9 days [13]. In a research by Lee et al. SDG was diagnosed 11.6 days after head injury [4]. In another Iranian study, the mean time of hygroma formation was 12.8 days [11]. Based on results of our study, SDG was formed in frontal and fronto-parietal areas more than other areas. In most patients (except one), most parts of hygroma was formed in frontal area. A less part was observed in other
parts of the brain. This can be the effect of earth gravity on brain. As most patients lie on their back, the shrunken brain gravitates toward occipital area and therefore, SDG is formed in frontal area [5]. In a study by Yousefzadeh-chabok et al. SDG was mostly observed in fronto-pareital area [11]. In our study, SDG was bilateral in most patients. Kim et al. reported the same in their study on children inflicted with SDG who underwent surgery [14]. Most accompanying cranial injuries in our patients had brain contusion followed by SAH. Liu et al. found similar results [12]. In Shinkei et al. study, most patients with SDG had other simultaneous cranial injuries such as contusion, SAH and ICH [15]. Accumulation of subdural fluid usually spontaneously disappears without urgent surgery [30]. Most of our patients underwent conservative treatment. Only two of them were operated due to SDG or subsequent chronic subdural hematoma (CSDH) due to SDG. In other studies on these patients, most of them underwent conservative treatment, only a few were operated [4,13]. Clinical outcome of patients was evaluated based on GOS and most of them had favorable outcome (good recovery, mild and moderate disability). In Lee et al. study, the outcome of patients were favorable in most cases (good recovery and mild disability) [4]. Of course, it is worthy of note that most patients under study had SDG with accompanying cranial injuries. Thus, intracranial injuries such as contusion, SAH, ICH, and the like can affect the final outcome of patients with traumatic SDG [15].

Figure 1. Subdural Hygroma Area
Conclusion
One of the lesions in trauma patients is SDG. We found SDG in trauma elderly patients, thus there is a need that prevention programs be devised to reduce the occurrence of trauma in this age group. Moreover, as this problem often disappears over time and most patients are eligible to undergo conservative treatment, surgery is not the best and most necessary solution. Thus, according to our findings and similar works, priotrizing medical care and treatments can reduce hospital costs and length of hospitalization after operation.
Acknowledgments
The authors would like to offer their special thanks to Clinical Research Development Unit of Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran.
Funding
None.
Conflicts of Interest
The authors declare no conflict of interest.
Author’s Contribution
Sharhokh Yousefzadeh-Chabok developed the original idea. Ali Babaei Jandaghi reviewed the manuscript for any probable challenge. Marieh Hosseinpour wrote the manuscript. Ali Babaei Jandaghi collected the data and co-authored. Ehsan Kazemnejad-Leili analyzed the data.
References
1. Ortiz-Prado E, Castillo TA, Lopez MO, Rubio MA, Bermeo LE. Post-Traumatic Subdural Hygroma: A One Year Follow up Case Report and Literature Review. Glob J Health Sci. 2016;8(12):239.
2. Patil AA, Bell B, Yamaguchi L. Drainage and Cranioplasty as a Treatment for Traumatic Subdural Hygroma Secondary to Decompressive Craniectomy. OJMN. 2016;6(01):41.
3. Yang X, Shen L, Lin QS, Li R, Quanmin N, Yongming Q. A Hypothesis of Traumatic Subdural Effusion Associated With Communicating Hydrocephalus in Infants and Its Management. J Craniofac Surg. 2015;26(2):435-7.
4. Lee KS, Bae WK, Bae HG, Yun IG. The fate of traumatic subdural hygroma in serial computed tomographic scans. J Korean Med Sci. 2000;15(5):560-8.
5. Lee K. The pathogenesis and clinical significance of traumatic subdural hygroma. Brain Inj. 1998;12(7):595-603.
6. Jeon SW, Choi JH, Jang TW, Moon S-M, Hwang H-S, Jeong JH. Risk factors associated with subdural hygroma after decompressive craniectomy in patients with traumatic brain injury: a comparative study. J Korean Neurosurg Soc. 2011;49(6):355-8.
7. Herold TJ, Taylor S, Abbrescia K, Hunter C. Post-traumatic subdural hygroma: case report. J. Emerg. Med. 2004;27(4):361-6.
8. Danil A. Posttraumatic extracerebral fluid collections. Rom. Neurosurg. 2013;20(2):139-48.
9. Coşar M, Eser O, Aslan A, Ela Y. Rapid resolution of acute subdural hematoma and effects on the size of existent subdural hygroma: a case report. Turk Neurosurg. 2007;17(3):224-7.
10. Tsuang F-Y, Huang AP-H, Tsai Y-H, Chen J-Y, Lee J-E, Tu Y-K, et al. Treatment of patients with traumatic subdural effusion and concomitant hydrocephalus: Clinical article. J Neurosurg. 2012;116(3):558-65.
11. Yousefzadeh-Chabok S, Hosseinpour M, Mohtasham-Amiri Z, Kazemnejad-Leili E, Alijani B. The Role of Surgical Treatment in Traumatic Subdural Hygroma: A Pilot Study. IrJNS. 2015;1(2):40-3.
12. Liu Y, Gong J, Li F, Wang H, Zhu S, Wu C. Traumatic subdural hydroma: clinical characteristics and classification. Injury. 2009;40(9):968-72.
13. Zanini MA, Resende LAdL, Freitas CCMd, Yamashita S. Traumatic subdural hygroma: five cases with changed density and spontaneous resolution. Arq. Neuro-Psiquiatr.. 2007;65(1):68-72.
14. Kim BO, Kim SW, Lee SM. Effectiveness of early surgery in children with traumatic subdural hygroma. J Korean Neurosurg Soc. 2005;37(6):432-5.
15. Zanini MA, de Lima Resende LA, de Souza Faleiros AT, Gabarra RC. Traumatic subdural hygromas: proposed pathogenesis based classification. Journal of Trauma and Acute Care Surgery. 2008;64(3):705-13.
| Rights and Permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information:
IrJNS Office, Guilan Road Trauma Research Center, Poursina Hospital, Namjoo St, Rasht, Guilan, Iran.
Publisher Tel : +9821 45355555 , 45355000
Email: ir.journalofneurosurgery@gmail.com, info@irjns.org
