


BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://irjns.org/article-1-81-en.html


 1, Iadh Ksira2 , Hichem Ben Selma3 , Abdelhafidh Slimane4 , Skander Korbi5 , Hamouda Guesmi3 , Hedi Krifa3
1, Iadh Ksira2 , Hichem Ben Selma3 , Abdelhafidh Slimane4 , Skander Korbi5 , Hamouda Guesmi3 , Hedi Krifa3
2- Assistant Professor of Neurosurgery, Sahloul Hospital, Department of Neurosurgery, Sousse, Tunisia
3- Professor of Neurosurgery, Sahloul Hospital, Department of Neurosurgery, Sousse, Tunisia
4- Intern of Neurosurgery, Sahloul Hospital, Department of Neurosurgery, Sousse, Tunisia
5- Assistant Professor of Anatomopathology, Farhat Hached Hospital, Department of Anatomopathology, Sousse, Tunisia
An Inflammatory Pseudotumor in the Costo-Vertebral Gutter: Case Report with Literature Review
Mourouj Mahfoudh 1*, Iadh Ksira 2, Hichem Ben Selma 3, Abdelhafidh Slimane 1, Skander Korbi 4, Hamouda Guesmi 3, Hedi Krifa 3
1 Intern of Neurosurgery, Sahloul Hospital, Department of Neurosurgery, Sousse, Tunisia
2 Assistant Professor of Neurosurgery, Sahloul Hospital, Department of Neurosurgery, Sousse, Tunisia
3 Professor of Neurosurgery, Sahloul Hospital, Department of Neurosurgery, Sousse, Tunisia
4 Assistant Professor of Anatomopathology, Farhat Hached Hospital, Department of Anatomopathology, Sousse, Tunis
* Corresponding Author Address: Department of Neurosurgery, Sahloul Hospital, Sousse, Tunisia. Tel: +21698452495. Fax: +21673330568. Email: Mourouj-mahfoudh@yahoo.com
Article Type: Case Report Received: December 14, 2016, Last Revised: March 6, 2017, Accepted: March 6, 2017, Published: March 31, 2017
Abstract
Background and Importance: Inflammatory pseudotumors are benign tumors-like lesions of unknown cause. The most familiar sites for inflammatory pseudotumors are the orbit and respiratory tract. An inflammatory pseudo tumor of costo-vertebral junction is rare.
Case Presentation: We presented here a 50-year-old male with two month history of progressive left cervico-brachial pain. The MRI showed an expansive process at the left costo-vertebral gutter with epidural extension through the lateral foramen, causing spinal cord compression from C7 to D3. The thoraco-abdominal CT scan did not identify other lesions.
Conclusion: The inflammatory pseudotumor is a chronic inflammatory process of unknown origin. The location of the costo-vertebral gutter is rare and the treatment involves sur gery, steroids and radiotherapy.
Keywords: Inflammatory Pseudotumor; Inflammatory Myofibroblastic Tumor; Magnetic Resonance Imaging; Costo-vertebral Junction; Biopsy
Please cite this paper as: Mahfoudh M, Ksira I, Ben Selma H, Slimane A, Korbi S, Guesmi H, Krifa H. An Inflammatory Pseudotumor in the Costo-Vertebral Gutter: Case Report with Literature Review. IrJNS. 2017;2(4):25-27
Background and Importance
Inflammatory pseudotumor (IPT) is a benign tumor-like lesion of unknown cause and is originally described in the lung and orbit, but it has recently been reported throughout the body and only a small number of people [1,3,6]. We presented a rare case of costo-vertebral inflammatory pseudotumor with epidural invasion presenting with progressive cervico-brachial pain. There were no signs of myelopathy.
Case Presentation
A 50-year-old male had a two month history of left cervicobrachial pain, with progressive weakness in left upper limb. The patient signed an informed written consent form before participation. The neurologic examination showed brachial monoparesis predominantly in distal left without pyramidal signs. Magnetic resonance imaging (MRI) showed hypointense lesion in both T1-and T2-weighed images (Figures 1,2) with intense contrast enhancement at the left costo-vertebral gutter with epidural extension through the lateral foramen, causing a compression on the spinal cord from C7 to D3 (Figure 3). The thoraco-abdominal CT scan did not show other lesions. A CT scan-guided biopsy through posterior-lateral approach was performed. The histological examination revealed that the lesion was made of dense collagen with fibrous background, associating fibroblastic or myofibroblastic cells having a clarified ovoid nuclei and inflammatory cells grouped into small clusters formed mainly of plasma cells and lymphocytes, and the lesion was richly vascularized. No necrosis was observed. The anti-actin smooth muscle antibody marked diffuse myofibroblasts that are H-caldesmone negative, the ALK was positive and the anti-cytokeratin AE1/AE3 antibody was negative excluding the possibility of an epithelial tumor. Hence, the diagnosis of an inflammatory pseudotumor was made.
Treatment started by steroids (1mg/kg/d) with adjuvant radiotherapy. There was a rapid recovery in his neurological functions, and there was a complete resolution of the lesion on control MRI after three years. There was no evidence of pulmonary or other lesions.
Discussion
Inflammatory pseudotumor was first described by Brunn in 1939 as a lesion in lung and was named as IPT by Umirker in 1954 [6,7]. It is a chronic inflammatory process of unknown origin and its histopathological presentation is very variable. It is most often located in the lungs and the orbit [1-4]. At the orbit, the inflammatory pseudotumor, is currently called idiopathic sclerosing inflammation [2]. Extra-pulmonary locations, apart from orbit are: nasal sinuses, liver, spleen, pancreas, intestine, kidney, urinary tract, bladder, testes, heart, and lymphatic system [1,5]. Only seven cases with epidural location in the spine have been reported to date [6]. In the nervous system, this condition is difficult to diagnose because its clinical and radiological presentation are not specific [2].
The IPT is hypointense in both T1 and T2-weighted MRI images showing strong enhancement with gadolinium contrast, as seen in our patient [1,4,6]. Histopathologically, the IPT includes inflammatory cell component made of plasma cells, phenotype B and T lymphocytes, histiocytes, eosinophils and macrophages sometimes taking a clear xanthomatous look [3,5,6]. It is associated to a fibroblast or myofibroblast component and a collagen background and more or less hyalinized [3,6]. Some inflammatory pseudotumors are found in association with immunoglobulin G4 (IgG4) related disease, a systemic immune-mediated fibrosclerosing disease characterized by IgG4-positive plasma cell [6,8]. The most used terms in recent literature are inflammatory pseudotumor and inflammatory myofibroblastic tumor, terms highlighting the importance of myofibroblasts in these lesions [3]. It is the case in our patient. Surgical excision is the best way to have a diagnosis and also is indicated for spinal cord decompression, although other treatments such as steroid therapy, antibiotics, radiotherapy, chemotherapy or CO2 laser have been tested on other locations of IPT with good results which can also reduce the size of the tumor [1,4,6]. Some authors consider IPT as inflammatory fibrosarcomas, and prognosis is an unfavorable result due to local and distant recurrence [3].
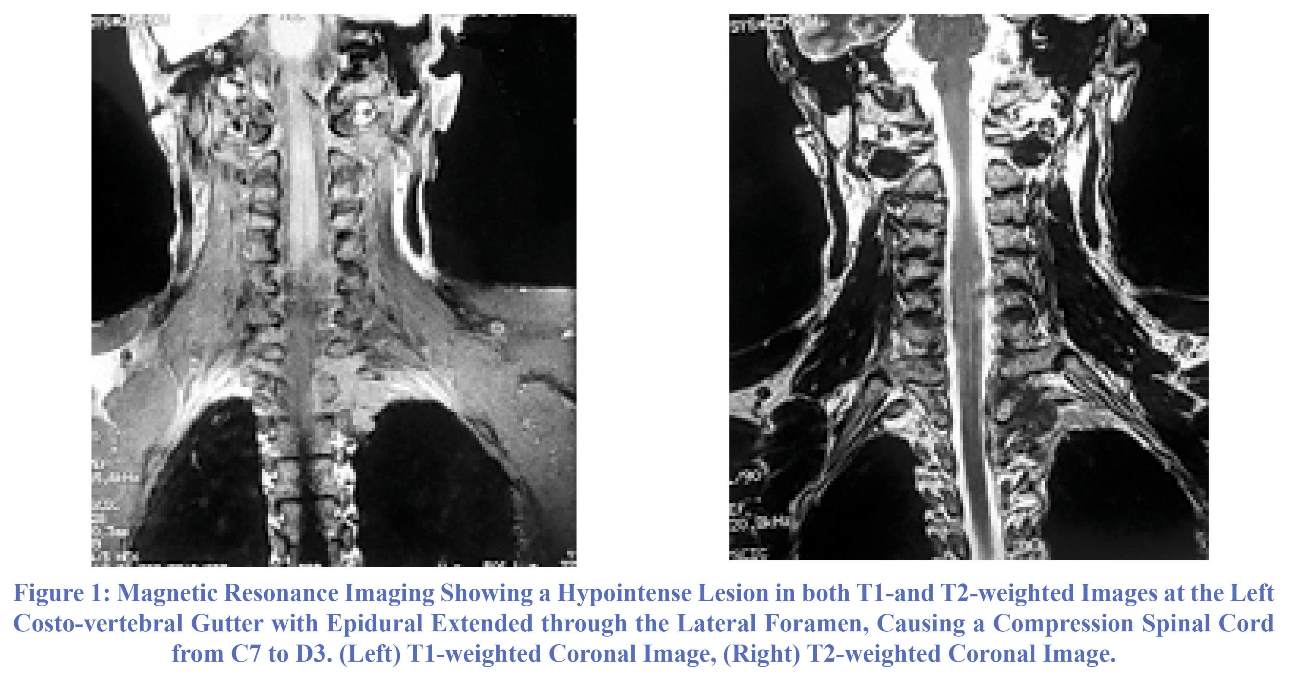
Figure 1: Magnetic Resonance Imaging Showing a Hypointense Lesion in both T1-and T2-weighted Images at the Left Costo-vertebral Gutter with Epidural Extended through the Lateral Foramen, Causing a Compression Spinal Cord from C7 to D3. (Left) T1-weighted Coronal Image, (Right) T2-weighted Coronal Image.
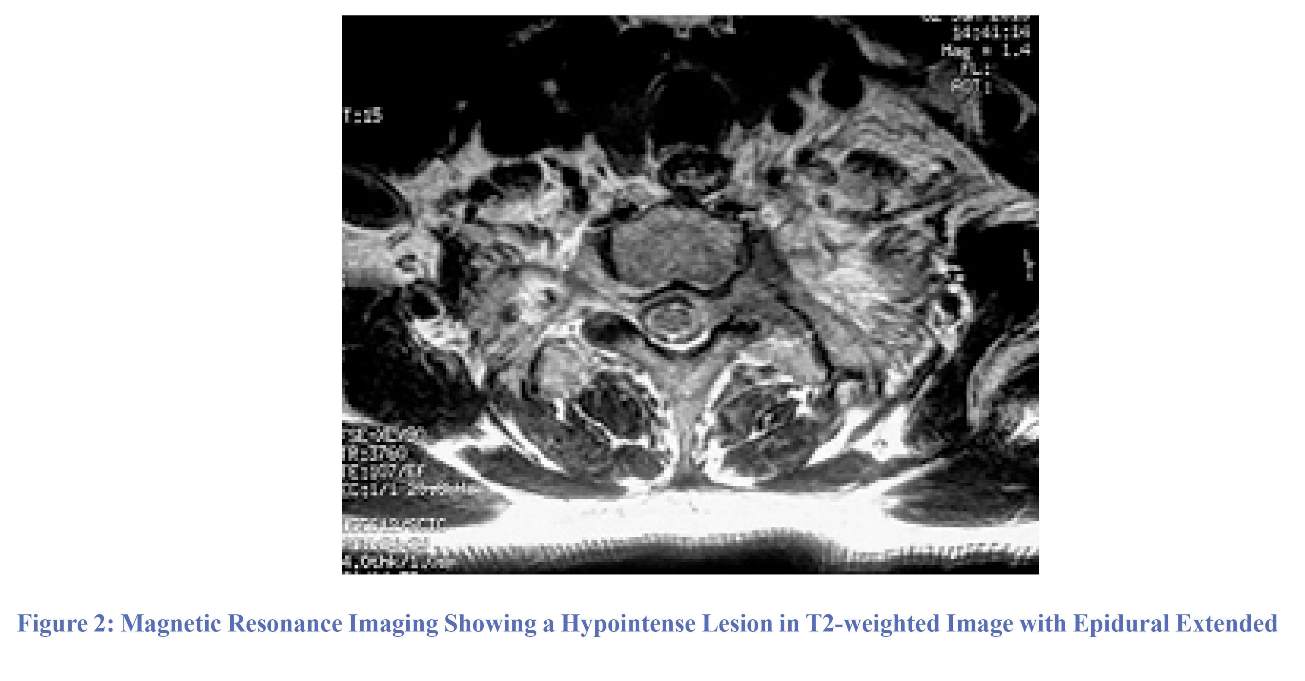
Figure 2: Magnetic Resonance Imaging Showing a Hypointense Lesion in T2-weighted Image with Epidural Extended

Figure 3: Magnetic Resonance Imaging Showing a Lesion in T1-weighted Image with Intense Contrast Enhancement at the Left Costo-vertebral Gutter with Epidural Extended through the Lateral Foramen, Causing a Compression Spinal Cord from C7 to D3. (Left) T1-weighted Coronal Image, (Right) T1-weighted Axial Image.
Conclusion
Inflammatory pseudotumor is mostly a benign myofibroblastic tumor of the soft tissue. Central nervous system involvement is a rare occurrence, and the costo-vertebral inflammatory pseudotumor with invasion of epidural space is rare. The CT guided biopsy confirmed the diagnosis. Treatment with steroid and adjuvant radiotherapy resulted in complete relief of the symptoms.
Funding
None.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Authors' Contribution
Conception and Design: Mourouj Mahfoudh
Data Collection: Mourouj Mahfoudh and Iadh Ksira
Drafting the Article: Mourouj Mahfoudh
Critically Revising the Article: All authors
Reviewing Submitted Version of Manuscript: All authors
Approving the Final Version of the Manuscript: All authors
References
1. Satoshi K, Hideki M, Satoru D, Katsuhito Y, Yoshiyuki O, Hiroyuki H. Epidural inflammatory pseudotumor in the thoracic spine in a patient with polymyalgia rheumatica. Spine J. 2012; 12(6):1-4.
2. El Jdid H, Sennaria FZ, Gueddari FZ, Imani F. Dural inflammatory pseudotumor: report of a single case. J neuradiol. 2010 ; 37(2):135-137.
3. Girard F, Kambouchner M, Maugendre S, Naccache JM, De Meyer-Cristiani R, Battesti JP. Pseudo-tumeurs inflammatoires pulmonaires d’évolution sévère. Rev Mal Resp. 2001 ; 18(5) :541-544.
4. Zemmoura I, Abderrahmane H, Morandi X. Intradural extramedullary spinal inflammatory myofibroblastic tumor: case report and literature review. Eur Spine J .2011; 20 (2):330-335.
5. Seol HJ, Kim SS, Kim JE, Lee SH, Won JY. Inflammatory Pseudotumor in the Epidural Space of the Thoracic Spine: A Case Report and Literature Review of MR Imaging Findings. Am J Neuroradiol. 2005; 26 (10):2667-2670.
6. Kanagaraju V, Rai D, Alluri RV, Prasanna C, Shyam Sundar V, Arvind Kumar SM. An inflammatory pseudotumor in the thoracic epidural space presenting with progressive paraplegia: a histopathological diagnosis with clinical and radiological uncertainty. Case report with literature review. Euro Spine J. 2016; 25 (1): 75-79.
7. Rack A, Belohradsky BH, Grantzow R, Schweinitz DV, Pfluger T, Kammer B. Inflammatory pseudotumor (IPT)-surgical cure of an inflammatory syndrome. Eur J Pediatr. 2016; 175 (7): 903-908.
8. Lai LM, McCarville MB, Kirby P, Kao SC, Moritani T, Clark E. Shedding light on inflammatory pseudotumor in children: spotlight on inflammatory myofibroblastic tumor. Pediatr Radiol 2015; 45 (12): 1738-1752.
| Rights and Permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information:
IrJNS Office, Guilan Road Trauma Research Center, Poursina Hospital, Namjoo St, Rasht, Guilan, Iran.
Publisher Tel : +9821 45355555 , 45355000
Email: ir.journalofneurosurgery@gmail.com, info@irjns.org
