Fri, Apr 19, 2024
Volume 4, Issue 4 (Autumn 2018)
Iran J Neurosurg 2018, 4(4): 225-232 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sharifi G, Mousavinejad S A, Dehghan M, Daneshmand khosravi Y, Ebrahimzadeh K, Samadian M et al . A Rare Intramedullary Epidermoid Cyst of the Thoracic Spinal Cord: Case Report and Review of Literature. Iran J Neurosurg 2018; 4 (4) :225-232
URL: http://irjns.org/article-1-155-en.html
URL: http://irjns.org/article-1-155-en.html
Guive Sharifi1 
 , Seyed ali Mousavinejad * 2, Mahmood Dehghan3 , Yahya Daneshmand khosravi4 , Kaveh Ebrahimzadeh1 , Mohammad Samadian5 , Omidvar Rezaie6
, Seyed ali Mousavinejad * 2, Mahmood Dehghan3 , Yahya Daneshmand khosravi4 , Kaveh Ebrahimzadeh1 , Mohammad Samadian5 , Omidvar Rezaie6
, Seyed ali Mousavinejad * 2, Mahmood Dehghan3 , Yahya Daneshmand khosravi4 , Kaveh Ebrahimzadeh1 , Mohammad Samadian5 , Omidvar Rezaie6
1- Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2- Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran , alimousavi65@yahoo.com
3- Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
5- Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
6- Department of Neurosurgery Loghman Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2- Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran , alimousavi65@yahoo.com
3- Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
5- Skull Base Research Center, Loghman Hakim Medical Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
6- Department of Neurosurgery Loghman Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Full Text [PDF 687 kb]
(1555 Downloads)
| Abstract (HTML) (4088 Views)




Full Text: (5041 Views)
1. Background and Importance
pidermoid cysts are rare tumors of spinal cord. Less than (1%) of all spinal cord tumors are epidermoid cysts [1], which are usually located as intradural and extramedullary and are products of developmental problems [2]. Sometimes they are iatrogenic [3]. As most of the reported cases are in thoracic and lumbar areas, there are few cases concerning thoracic intramedullary epidermoid cysts. Here, we report a case of small intramedullary epidermoid cyst in a 40 year-old woman.
2. Case Presentation
A forty-two year-old woman was referred to our clinic for radicular pain and weakness in left extremity. The patient had no other complaints. Physical examinations including neurological examination of cranial nerves and upper extremities were normal. Hyperactive reflexes and spasticity of the lower extremities were noted. Bilateral Babinski responses were elicited. The muscle strength of the lower extremities was diminished, especially in distal muscles and the weakness was more in the left in contrast to the right side of the body. No definite sensory level was found. A sense of position and vibratory sensations were preserved. The anal reflex was normal.
On lumbosacral MRI, a left paracentral L5-S1 disk protrusion was seen; however, it could not justify the symptoms on her right lower extremity. Therefore, MRI of cervical and thoracic spines were requested. Cervical MRI findings were normal. Thoracic MRI illustrated a focal fusiform enlargement of the thoracic cord at T4 and T5. On sagittal images, hypointensive and hyperintensive intramedullary lesions at T4 level were seen on T1 and T2-weighted images, respectively (figure 1 A & B, figure 2). The cord above and below this cavity tapered down to a normal diameter and did not show abnormal signal. The lesion did not show any enhancement in MRI with gadolinium (figure 1 C).
pidermoid cysts are rare tumors of spinal cord. Less than (1%) of all spinal cord tumors are epidermoid cysts [1], which are usually located as intradural and extramedullary and are products of developmental problems [2]. Sometimes they are iatrogenic [3]. As most of the reported cases are in thoracic and lumbar areas, there are few cases concerning thoracic intramedullary epidermoid cysts. Here, we report a case of small intramedullary epidermoid cyst in a 40 year-old woman.
2. Case Presentation
A forty-two year-old woman was referred to our clinic for radicular pain and weakness in left extremity. The patient had no other complaints. Physical examinations including neurological examination of cranial nerves and upper extremities were normal. Hyperactive reflexes and spasticity of the lower extremities were noted. Bilateral Babinski responses were elicited. The muscle strength of the lower extremities was diminished, especially in distal muscles and the weakness was more in the left in contrast to the right side of the body. No definite sensory level was found. A sense of position and vibratory sensations were preserved. The anal reflex was normal.
On lumbosacral MRI, a left paracentral L5-S1 disk protrusion was seen; however, it could not justify the symptoms on her right lower extremity. Therefore, MRI of cervical and thoracic spines were requested. Cervical MRI findings were normal. Thoracic MRI illustrated a focal fusiform enlargement of the thoracic cord at T4 and T5. On sagittal images, hypointensive and hyperintensive intramedullary lesions at T4 level were seen on T1 and T2-weighted images, respectively (figure 1 A & B, figure 2). The cord above and below this cavity tapered down to a normal diameter and did not show abnormal signal. The lesion did not show any enhancement in MRI with gadolinium (figure 1 C).
Operative Approach
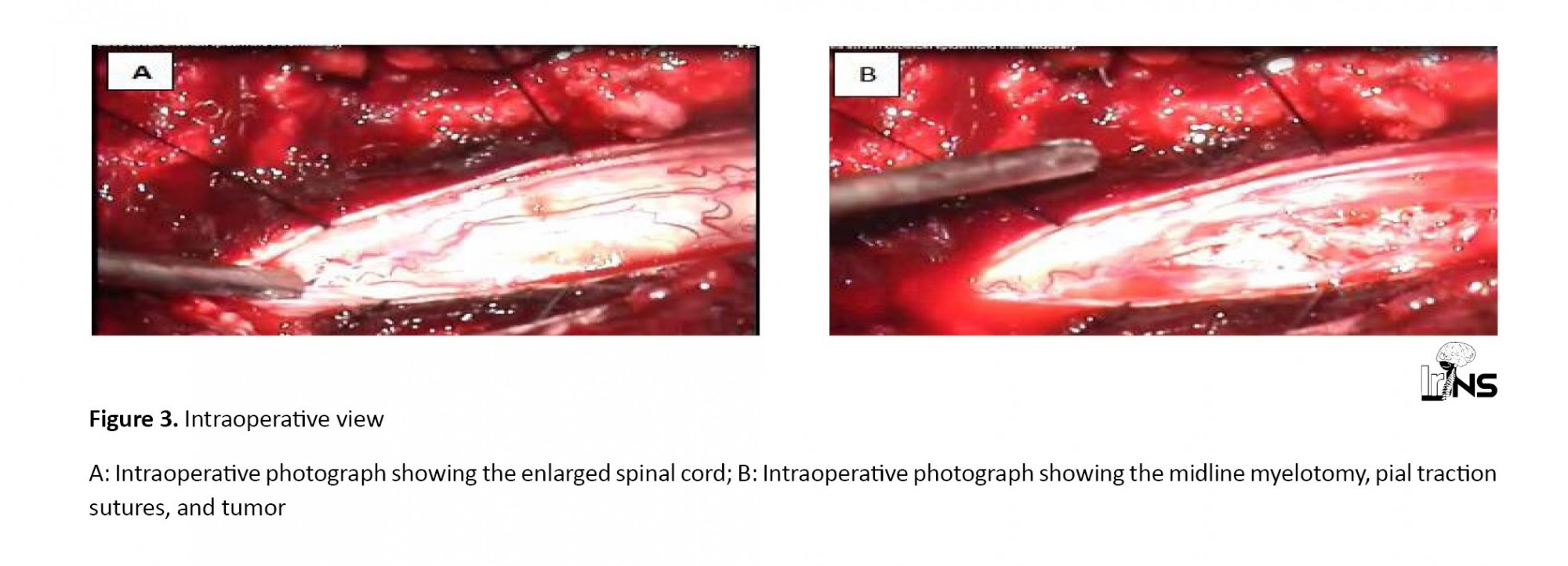
A laminectomy (T3-T5) was performed and no evidence of dysraphism such as a dermal sinus, was found. When the dura was opened, the cord appeared distended (figure 3 A). Under the operating microscope, the posterior median raphe was obliterated and the midline was identified at the midpoint between the dorsal root entry zones. A 1.5-cm myelotomy centered over the lesion was performed (figure 3 B). There was an avascular mass lying completely within the cord immediately beneath the surface. Pia traction sutures were used to open the myelotomy incision and expose the intramedullary tumor. The mass consisted of a white, waxy, and flaky material with no apparent skin appendages. The tumor was gradually and completely removed and the cord was decompressed. No attempt was made to remove the lining of the cyst since it was firmly attached to the substance of the cord.
A laminectomy (T3-T5) was performed and no evidence of dysraphism such as a dermal sinus, was found. When the dura was opened, the cord appeared distended (figure 3 A). Under the operating microscope, the posterior median raphe was obliterated and the midline was identified at the midpoint between the dorsal root entry zones. A 1.5-cm myelotomy centered over the lesion was performed (figure 3 B). There was an avascular mass lying completely within the cord immediately beneath the surface. Pia traction sutures were used to open the myelotomy incision and expose the intramedullary tumor. The mass consisted of a white, waxy, and flaky material with no apparent skin appendages. The tumor was gradually and completely removed and the cord was decompressed. No attempt was made to remove the lining of the cyst since it was firmly attached to the substance of the cord.
The material was sent to a pathologist and the diagnosis of epidermoid cyst was confirmed (figure 4). The patient was visited two weeks later and no symptoms in the left side of the body were seen. The MRI of the brain was normal with no sign of myelin degenerative diseases like multiple sclerosis.
3. Discussion
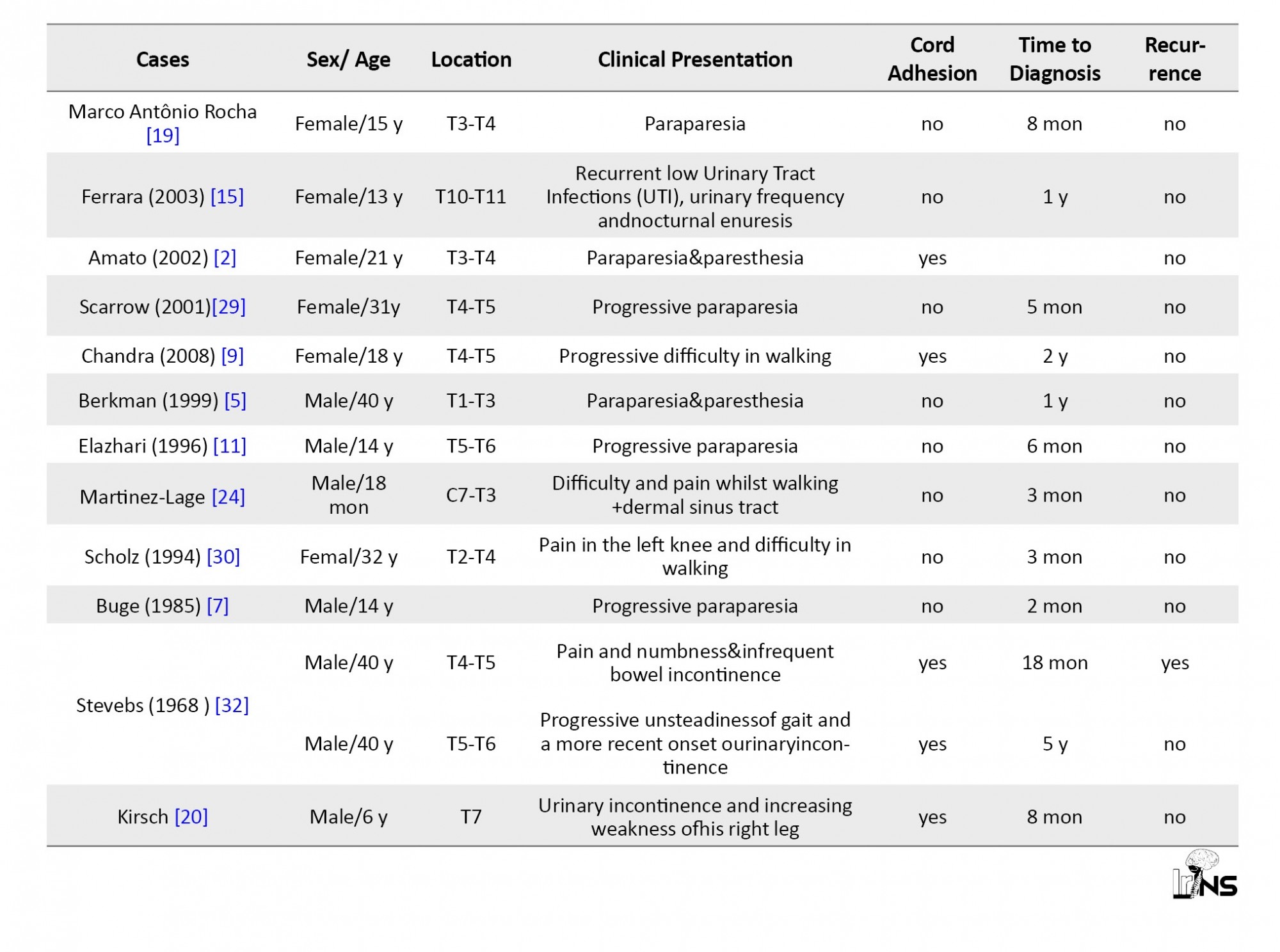
Less than (1%) of intraspinal tumors are epidermoid cysts. These benign tumors are very rare with cranial to spinal ratio of 14:1 [4]. Pure intramedullary epidermoid cycts are rare and only 32 cases of intramedullary cysts in thoracic cord are reported (table 1). Epidermoid cyst is the result of incomplete cleavage of the neural ectoderm from cutaneous ectoderm within the third to fifth week of gestation [5]. It is usually a developmental problem but iatrogenic cases due to implanting epidermal cells by repetitive lumbar puncture are also reported [3]. MRI is the diagnostic measure to detect the cyst with absence of peri-tumor edema and sharp borders differentiating tumor from normal tissue [6]. The preferred treatment of epidermoid cyst is complete removal. however there is a report of several recurrences in the same location [7]. Although these tumors are essentially considered benign, malignant transformation might be seen [8].
Less than (1%) of intraspinal tumors are epidermoid cysts. These benign tumors are very rare with cranial to spinal ratio of 14:1 [4]. Pure intramedullary epidermoid cycts are rare and only 32 cases of intramedullary cysts in thoracic cord are reported (table 1). Epidermoid cyst is the result of incomplete cleavage of the neural ectoderm from cutaneous ectoderm within the third to fifth week of gestation [5]. It is usually a developmental problem but iatrogenic cases due to implanting epidermal cells by repetitive lumbar puncture are also reported [3]. MRI is the diagnostic measure to detect the cyst with absence of peri-tumor edema and sharp borders differentiating tumor from normal tissue [6]. The preferred treatment of epidermoid cyst is complete removal. however there is a report of several recurrences in the same location [7]. Although these tumors are essentially considered benign, malignant transformation might be seen [8].
In our patient, the small epidermoid cyst at T4 was the culprit causing symptoms. The epidermoid cyst may be accompanied by a dermal lesion, which was absent in our case. After surgery, the patient was symptom free as the pressure on the cord was removed. In an 18-month follow-up, no symptom was seen.
In patients with symptoms and signs of upper and lower motor neuron, before labelling the patient with a disease only according to brain MRI findings, a careful imaging study of the spinal cord might be reasonable. In other words, lesions in thoracic region of the spinal cord are usually neglected because of another lesion in the lumbosacral imaging that might justify the symptoms. As in our case, a small intramedullary lesion can mimic the signs and symptoms of more serious diseases like multiple sclerosis. The small size of tumor in our patient and normal skin over the thoracic cord in concert with few neurologic symptoms which were to some degree justified by patient’s brain MRI had led to misdiagnosis of the condition.
Review of the Literature
Review of the literature was performedusing PubMed database by searching for the following combinations: “Epidermoid cyst” AND “spinal cord”. The search was limited to humans and articles reported in English. No restriction was set regarding the type of publication, the publication date, or publication status. The search was broadened extensively cross-checking the reference lists of all retrieved articles fulfilling the aim of the study. For all databases, the latest date of search was run on 2018.
Thirty-two cases of reports belonged to years of publication from 1965 to 2018. Table 1 lists all of the cases reported in the literature with epidermoid cyst” and “spinal cord”. the patient's age ranged from 16 months to 74 years old. one patient presented with fever and recurrent upper respiratory tract infection [16]. two patients presented with sudden paresia [9, 19]. Twenty-eight cases of 32 progressive paraparesia were observed. Back pain was observed in seven cases [10, 11, 15, 19, 20, 22, 26].
In two cases, clinical symptoms occurred in less than three years [9, 16, 31]. They were often referred to a clinic with more severe symptoms and abrupt onset symptoms. In 17 of 32 cases (53%), urinary tract symptoms such as urinary incontinence and bladder disorders were observed. in one patient, the only symptom was recurrent urinary tract infection and incontinency [25]. All cases of involvement included the thoracic area in the imaging. In 20 patients (62.5%) of cases, the onset of the complications was reported to be at least Six months. In two patients, thoracic intramedullary epidermoid cysts coexisted with sinus dermal tract diagnosed before reaching theee years old of age whereas in one history of meningocele, surgery in thoracic region was reported [35].
In 19 patients, the total resection of tumor with tumor capsule excision were achieved but in 13 patients the capsules were adherent to spinal cord and partial resection of capsule was performed. Tree patients (8, 16, 34) underwent second surgery for tumor recurrent. in two of them, subtotal resection of tumor was done because of capsule adhesion to spinal cord [16, 34]. One patient with malignant transformation of epidermoid cyst was reported [8].
4. Conclusion
Spinal intramedullary epidermoid cysts are rare tumors without specific clinical presentation. The recognition of epidermoid cysts in the pediatric age group is important. There may be associated congenital anomalies which need to be carefully sought as an aid to diagnosis. Early diagnosis can be done by MRI. Surgical excision is the treatment of choice and the overall outcome of these lesions is good, even if they present with a ruptured cyst, as was the case with our patient.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages; they were also assured about the confidentiality of their information; Moreover, They were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
In patients with symptoms and signs of upper and lower motor neuron, before labelling the patient with a disease only according to brain MRI findings, a careful imaging study of the spinal cord might be reasonable. In other words, lesions in thoracic region of the spinal cord are usually neglected because of another lesion in the lumbosacral imaging that might justify the symptoms. As in our case, a small intramedullary lesion can mimic the signs and symptoms of more serious diseases like multiple sclerosis. The small size of tumor in our patient and normal skin over the thoracic cord in concert with few neurologic symptoms which were to some degree justified by patient’s brain MRI had led to misdiagnosis of the condition.
Review of the Literature
Review of the literature was performedusing PubMed database by searching for the following combinations: “Epidermoid cyst” AND “spinal cord”. The search was limited to humans and articles reported in English. No restriction was set regarding the type of publication, the publication date, or publication status. The search was broadened extensively cross-checking the reference lists of all retrieved articles fulfilling the aim of the study. For all databases, the latest date of search was run on 2018.
Thirty-two cases of reports belonged to years of publication from 1965 to 2018. Table 1 lists all of the cases reported in the literature with epidermoid cyst” and “spinal cord”. the patient's age ranged from 16 months to 74 years old. one patient presented with fever and recurrent upper respiratory tract infection [16]. two patients presented with sudden paresia [9, 19]. Twenty-eight cases of 32 progressive paraparesia were observed. Back pain was observed in seven cases [10, 11, 15, 19, 20, 22, 26].
In two cases, clinical symptoms occurred in less than three years [9, 16, 31]. They were often referred to a clinic with more severe symptoms and abrupt onset symptoms. In 17 of 32 cases (53%), urinary tract symptoms such as urinary incontinence and bladder disorders were observed. in one patient, the only symptom was recurrent urinary tract infection and incontinency [25]. All cases of involvement included the thoracic area in the imaging. In 20 patients (62.5%) of cases, the onset of the complications was reported to be at least Six months. In two patients, thoracic intramedullary epidermoid cysts coexisted with sinus dermal tract diagnosed before reaching theee years old of age whereas in one history of meningocele, surgery in thoracic region was reported [35].
In 19 patients, the total resection of tumor with tumor capsule excision were achieved but in 13 patients the capsules were adherent to spinal cord and partial resection of capsule was performed. Tree patients (8, 16, 34) underwent second surgery for tumor recurrent. in two of them, subtotal resection of tumor was done because of capsule adhesion to spinal cord [16, 34]. One patient with malignant transformation of epidermoid cyst was reported [8].
4. Conclusion
Spinal intramedullary epidermoid cysts are rare tumors without specific clinical presentation. The recognition of epidermoid cysts in the pediatric age group is important. There may be associated congenital anomalies which need to be carefully sought as an aid to diagnosis. Early diagnosis can be done by MRI. Surgical excision is the treatment of choice and the overall outcome of these lesions is good, even if they present with a ruptured cyst, as was the case with our patient.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages; they were also assured about the confidentiality of their information; Moreover, They were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
- Rahman MA, Chaurasia BK, Hossain MA, Habib S, Barua KK. Very rare upperdorsal intramedullary epidermoid with paraplegia: a case report. Neuroimmunology and Neuroinflammation. 5, 14. [DOI:10.20517/2347-8659.2017.57]
- Amato VG, Assietti R, Arienta C. Intramedullary epidermoid cyst: Preoperative diagnosis and surgical management after MRI introduction: Case report and updating of the literature/comments. Journal of neurosurgical sciences. 2002; 46(3/4):122.
- Babayev R, Abbasov B, Ekşi MŞ. Thoracic intramedullary epidermoid cyst-timely fashion diagnosis and treatment. Child's Nervous System. 2015; 31(5):793-6. [DOI:10.1007/s00381-015-2625-6] [PMID]
- Berger MS, Wilson CB. Epidermoid cysts of the posterior fossa. Journal of neurosurgery. 1985; 62(2):214-9. [DOI:10.3171/jns.1985.62.2.0214] [PMID]
- Berkman Z, İplikçioğlu C, Bek Ş, Özcan D. Intramedullary epidermoid tumors: A report of two cases. Marmara Medical Journal. 1999; 12(1):39-42.
- Buge A, Chamouard JM, Schadeck B, Sichez JP, Fabiani JM. 1985. [Spinal cord congenital epidermoid cyst (a dorsal case)]. Rev Neurol (Paris). 1985; 141(12):810-3. [PMID]
- Çataltepe O, Berker M, Akalan N. A giant intramedullary spinal epidermoid cyst of the cervicothoracic region. Pediatric neurosurgery. 2004; 40(3):120-3. [DOI:10.1159/000079853] [PMID]
- Chandra PS, Manjari T, Devi BI, Chandramouli BA, Srikanth SG, Shankar SK. Intramedullary spinal epidermoid cyst. Neurology India. 2000; 48(1):75.
- Cincu R, Lazaro JF, Liesa JL, Callizo JR. Dorsal intramedullary spinal epidermoid cysts: Report of two cases and review of literature. Indian journal of orthopaedics. 2007; 41(4):395. [DOI:10.4103/0019-5413.37005] [PMID] [PMCID]
- Elazhari A, Sami A, Naja A, Ouboukhlik A, Elkamar A, Boucetta M. A thoracic medullary epidermoid cyst. A case report with MRI and literature review. Neurochirurgie. 1996; 42(6):309-11.
- Faheem M, Zeeshan Q, Ojha BK, Chandra A, Singh SK, Srivastava C, et al. Isolated thoracic intramedullary epidermoid cyst-a rare entity. Romanian Neurosurgery. 2016; 30(2):272-3. [DOI:10.1515/romneu-2016-0042]
- Fazio MG, Kil AM, Rooks VJ, Biega TJ. Diffusion-weighted magnetic resonance imaging of an intramedullary epidermoid cyst with dorsal dermal sinus tract in a toddler. Case Rep Radiol, 2013; 878713. [DOI:10.1155/2013/878713] [PMID] [PMCID]
- Fereydoonian NA, Bakhti S, Fereshtehnejad SM, Tabibkhooei AR. Intramedullary thoracic spine epidermoid cyst with myelopathic presentations: a report of a rare case. Clinical neurology and neurosurgery. 2013; 6(115):841-3.[DOI:10.1016/j.clineuro.2012.08.002] [PMID]
- Ferrara P, Costa S, Rigante D, Mule A, D'Aleo C, Pulitano S, Belli P, Menchinelli P, Caldarelli M. Intramedullary epidermoid cyst presenting with abnormal urological manifestations. Spinal cord. 2003; 41(11):645. [DOI:10.1038/sj.sc.3101482] [PMID]
- Fleming C, Kaliaperumal C, O’Sullivan M. Recurrent intramedullary epidermoid cyst of conus medullaris. BMJ case reports. 2011; 2011:bcr1120115090. [DOI:10.1136/bcr.11.2011.5090] [PMID] [PMCID]
- Gonzalvo A, Hall N, McMahon JH, Fabinyi GC. Intramedullary spinal epidermoid cyst of the upper thoracic region. Journal of Clinical Neuroscience. 2009; 16(1):142-4.[DOI:10.1016/j.jocn.2008.04.017] [PMID]
- Graillon T, Rakotozanany P, Meyer M, Dufour H, Fuentes S. Intramedullary epidermoid cysts in adults: Case report and updated literature review. Neurochirurgie. 2017; 63(2):99-102. [DOI:10.1016/j.neuchi.2017.01.004] [PMID]
- Júnior MA, de Carvalho GT, Faria MP, Faglioni Jr W, de Souza AA. Tumor epidermóide intramedular: relato de caso. Arquivo brasileiro de Neuropsiquiatria. 2003; (61):867-9.
- Kirsch WM, Hodges FJ. An intramedullary epidermal inclusion cyst of the thoracic cord associated with a previously repaired meningocele: case report. Journal of neurosurgery. 1966; 24(6):1018-20. [DOI:10.3171/jns.1966.24.6.1018] [PMID]
- Kumar M, Malgonde MS, Kumar SA. Thoracic intramedullary spinal epidermoid tumor: A rare entity. Saudi Journal for Health Sciences. 2013; 2, 132. [DOI:10.4103/2278-0521.117920]
- Lee JH, Shin JJ, Hwang YS, Kim TH, Shin HS, Park SK. Intramedullary Epidermoid Cyst in Thoracolumbar Junctiont: A Case Report. Korean J Spine. 2008; 5(3):219-24.
- Manno NJ, Uihlein A, Kernohan JW. Intraspinal epidermoids. Journal of neurosurgery. 1962; 19(9):754-65. [DOI:10.3171/jns.1962.19.9.0754] [PMID]
- Martínez-Lage JF, Esteban JA, Poza M, Casas C. Congenital dermal sinus associated with an abscessed intramedullary epidermoid cyst in a child: case report and review of the literature. Child's nervous system. 1995; 11(5):301-5.
- Mishra SS, Satapathy MC, Deo RC, Tripathy SR, Senapati SB. Isolated thoracic (D5) intramedullary epidermoid cyst without spinal dysraphism: A rare case report. Journal of pediatric neurosciences. 2015; 10(2):133.
- Munshi A, Talapatra K, Ramadwar M, Jalali R. Spinal epidermoid cyst with sudden onset of paraplegia. Journal of cancer research and therapeutics. 2009; 5(4):290.[
- Ogden AT, Khandji AG, McCormick PC, Kaiser MG. Intramedullary inclusion cysts of the cervicothoracic junction: report of two cases in adults and review of the literature. Journal of Neurosurgery: Spine. 2007; 7(2):236-42. [DOI:10.3171/SPI-07/08/236] [PMID]
- Alves AM, Norrell H. Intramedullary epidermoid tumors of the spinal cord. Report of a case and review of the literature. International surgery. 1970; 54(4):239. [PMID]
- Scarrow AM, Levy EI, Gerszten PC, Kulich SM, Chu CT, Welch WC. Epidermoid cyst of the thoracic spine: case history. Clinical neurology and neurosurgery. 2001; 103(4):220-2. [DOI:10.1016/S0303-8467(01)00156-1]
- Scholz M, Märzheuser-Brands S, Gottschalk J, Böck JC, Lanksch WR. Intramedullary epidermoid cyst. A case report. Neurosurgical review. 1994; 17(1):89-93. [DOI:10.1007/BF00309994] [PMID]
- Somasundaram A, Lesser GJ, Mott RT, Hsu W. Malignant transformation of an intramedullary epidermoid cyst in the thoracic region of the spinal cord: Case report. Journal of Neurosurgery: Spine. 2013; 19(5):591-4. [DOI:10.3171/2013.8.SPINE13150] [PMID]
- Stevens WW, Schlesinger EB. Intramedullary epidermoid tumors of the thoracic spinal cord: Report of two cases. Journal of neurosurgery. 1968; 29(3):296-9. [DOI:10.3171/jns.1968.29.3.0296] [PMID]
- Swamy MN. A Case of intramedullar epidermoid cyst. Medical journal, Armed Forces India. 2008; 64(1):72.[DOI:10.1016/S0377-1237(08)80155-4]
- Wang M, Wu T, Chen J, Tsai T, Chen T, Tzeng W, Chang J, Su C. Magnetic resonance imaging of intramedullary epidermoid cyst of low thoracic spinal cord: a case report. Chinese Journal of Radiology-Taipei. 2005; 30(2):109.
- Yen CP, Kung SS, Kwan AL, Howng SL, Wang CJ. Epidermoid cysts associated with thoracic meningocele. Acta neurochirurgica. 2008; 150(3):305-9. [DOI:10.1007/s00701-007-1398-4] [PMID]
- Zavanone M, Guerra P, Rampini PM, Crotti F, Vaccari U. A cervico-dorsal intramedullary epidermoid cyst. Case report and review of the literature. Journal of neurosurgical sciences. 1991; 35(2):111-5.
Type of Study: Case report |
Send email to the article author
| Rights and Permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Articles Copyright © The Author(s).
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information:
IrJNS Office, Guilan Road Trauma Research Center, Poursina Hospital, Namjoo St, Rasht, Guilan, Iran.
Publisher Tel : +9821 45355555 , 45355000
Email: ir.journalofneurosurgery@gmail.com, info@irjns.org
Owned by Guilan University of Medical Sciences.
Co-published by Negah Institute for Scientific Communication.
Contact Information:
IrJNS Office, Guilan Road Trauma Research Center, Poursina Hospital, Namjoo St, Rasht, Guilan, Iran.
Publisher Tel : +9821 45355555 , 45355000
Email: ir.journalofneurosurgery@gmail.com, info@irjns.org
