Wed, Jun 24, 2026
Volume 11 - Continuous Publishing
Iran J Neurosurg 2025, 11 - Continuous Publishing: 0-0 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Garshasbi S, Emami-Razavi S H, Saffarinia M, Elmi Manesh N. The Role of Defensive Mechanisms on Emotional Expressiveness and Symptoms of Social Anxiety Disorder in Spinal Cord-injured Patients. Iran J Neurosurg 2025; 11 : 28
URL: http://irjns.org/article-1-337-en.html
URL: http://irjns.org/article-1-337-en.html



1- Brain and Spinal Cord Injury Research Center, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran. & 2. Department of Health in Emergencies and Disasters, School of Public Health, Tehran University of Medical Sciences, Tehran, Iran , sgarshasbi@farabi.tums.ac.ir
2- Brain and Spinal Cord Injury Research Center, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran. & Department of Surgery, Imam Khomeini Hospital Complex, Tehran University of Medical Sciences, Tehran, Iran.
3- Department of Psychology, Payame Noor University, Tehran, Iran
4- Department of Psychology, Payam Noor University, Tehran, Iran.
2- Brain and Spinal Cord Injury Research Center, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran. & Department of Surgery, Imam Khomeini Hospital Complex, Tehran University of Medical Sciences, Tehran, Iran.
3- Department of Psychology, Payame Noor University, Tehran, Iran
4- Department of Psychology, Payam Noor University, Tehran, Iran.
Keywords: Social anxiety disorder, Spinal cord injury (SCI), Defensive mechanisms, Descriptive correlational study
Full Text [PDF 899 kb]
(151 Downloads)
| Abstract (HTML) (505 Views)
Full Text: (101 Views)
1. Introduction
Spinal cord injury (SCI) is defined as any damage to the spinal cord that can result from either trauma or disease. The majority of the spinal injuries result from trauma (90%). The symptoms of spinal injury depend on the severity of the injury and its location. The SCI signs include loss of sensation and control of leg and hand movements. The most severe SCI occurs when the systems regulating the functions of the intestines, the bladder, the respiratory system, the heartbeat, and blood pressure are disturbed. Most spinal cord-injured patients suffer chronic pain [1]. The World Health Organization (WHO) estimates that the global incidence of SCI is 40-80 cases in every million individuals. SCI prevalence in Iran is estimated to be virtually 40-50 cases in every million individuals [2]. Some secondary complications accompany SCI, which can be disabling and even threaten life. Among secondary complications are deep vein thrombosis (DVT), urinary system infections, muscular spasms, osteoporosis, chronic pain, and respiratory consequences [3].
SCI can result in serious hygienic, physical, and social impacts on affected patients, imposing considerable negative effects on their quality of life [4]. Along with physical consequences of SCI, it is estimated that 20-30% of the patients will experience symptoms of depression, which has a negative influence on the function and general health. Besides, SCI leads to mental situations such as anxiety, identity disturbance, and feeling lonely. Moreover, suicide, drug abuse, and separation are more frequent in these patients compared to normal persons [3]. The prevalence of depression and anxiety in SCI patients is reported as 30-40% and 20-25%, respectively [5]. One of the significant negative impacts on SCI patients is changes in life quality and its resulting psychological complications [6]. The stress as a result of SCI disability makes the patients isolated and socially detached. Consequently, the patients get depressed and feel incompetent. Nowadays, emotional health is considered one of the most important pillars of health.
Accordingly, emotional health is stated as emotional perception and the ability to cope with everyday life issues. An emotionally healthy person correctly distinguishes his emotions and expresses them in appropriate situations [7]. Emotional expressiveness is defined as an external display of emotion, regardless of its positive or negative value, whether expressed verbally or physically. People express their emotions differently. Some individuals express their emotions freely without considering the consequences, a trait called emotional expressiveness. Nevertheless, some adopt a conservative approach and do not express their emotions. In some others, inhibition of emotions leads to mental confusion and even physical problems in them, and these people suffer from emotional inhibition [7].
The emotion has 4 functions: organizing excitement, fostering self-understanding, improving coping skills, and strengthening interpersonal relationships [8]. According to King and Emmons, emotional expression does not necessarily indicate health; rather, the person’s feelings toward these expressive behaviors indicate the health. To express the emotional role of health, three emotional expression dimensions are considered: negative expression, positive expression, and sincerity expression [9]. Several studies have been conducted in this field and demonstrate a relationship between emotional expressiveness and some physical illnesses like cancer and cardiovascular diseases [7]. A positive relationship between positive emotional expression and psychological well-being was reported by Kennedy-Moore and Watson [8]. Misconception, negative attitude, and physical obstacles lead to a considerable deprivation in spinal cord-injured patients, which does not permit their active participation in society. For instance, children with SCI start school later compared to their peers and even progress more slowly at school. Likewise, people with physical disabilities make fewer social contacts and have a great tendency to loneliness and isolation compared to ordinary persons [10]. Social anxiety disorder or social phobia is a disabling disorder that can influence a considerable portion of society [11]. In fact, social phobia disorder is the most prevalent disorder in childhood and adolescence [3]. According to Rapee, social anxiety disorder includes a wide range of anxiety: No social anxiety, normal level of social anxiety, social anxiety (low level of shame), fears and social avoidances (social anxiety disorder), pervasive level of social anxiety disorder, and avoidant personality disorder [12].
Defense mechanisms are unconscious mental processes that protect against different kinds of anxiety. These mechanisms not only protect individuals against anxiety and warn about possible dangers and internal stressors but also regulate mental experiences related to painful thoughts, feelings, and emotions [13]. According to Vailnat’s hierarchical classification, defensive mechanisms are divided into 20 mechanisms in 3 defensive styles: mature defense styles, immature defense styles, and neuroticism. Mature defensive mechanisms are considered adaptive, normal, and efficient coping styles, while immature and neurotic defensive mechanisms are nonadaptive and inefficient coping styles. Notably, people adopt different defensive styles in specific situations [14].
Until now, several studies have been carried out on defensive mechanisms, emotional expression, and social anxiety disorder for different target groups who deal with chronic diseases. Nonetheless, defensive mechanisms in individuals with SCI have not been fully evaluated in Iran. The current study aims to investigate the role of defensive mechanisms on emotional expression and symptoms of social anxiety disorder in SCI patients. Eventually, we hope the findings of this investigation help SCI patients receive the necessary education and therapeutic interventions, such as emotional expression, defensive mechanisms, etc. to prevent social anxiety disorder in them.
2. Methods and Materials/Patients
The study sample
The current study, which began in April 2023 and lasted 1 year, was descriptive, correlational, and survey-based. The study population consisted of SCI patients who were referred to the medical centers of the State Welfare Organization of Tehran Province. Initially, ethical approval was obtained to conduct this study. Then, the patients were invited verbally to participate in our investigation. The sample size was determined using G*Power software, version 3.1 with a type I error (false positive) rate of 5%, a power of 80%, and a medium effect size of 0.6, yielding a sample size of 115. The inclusion criterion was adults with SCI and literacy. The exclusion criteria were failure to meet the inclusion criteria and unwillingness to participate in the study.
The questionnaires were distributed to 115 participants, and at the end, 100 were completed; 15 patients dropped out during the study. Demographic characteristics of the participants were as follows: 31 women and 69 men; 56.7% married and 40.2% single; 6.2% with undergraduate education, 57.7% with diploma education, and 32% with university education. According to the levels of SCI, 44.3% had lumbar, 36.1% cervical, and 17.5% thoracic injuries.
Study questionnaires
To collect the research findings, the defense style questionnaire (DSQ), the emotional expressiveness questionnaire (EEQ), and the social phobia inventory (SPI) were employed. DSQ was prepared by Andrews and colleagues [15]. It is scored on a Likert scale and consists of 40 questions, each assessing 20 defensive mechanisms across 3 levels: Undeveloped, developed, and neuroticism. For each defensive mechanism, the score ranges from 2 to 18. Scores >10 indicate that the person uses this mechanism. In each defensive style, a person’s average score indicates the defensive mechanism he uses; the highest score indicates the defensive style he uses. The internal reliability of this instrument has been reported to range from 0.75 to 0.85 across studies, and its factor structure has been confirmed across several versions (including DSQ-40 and DSQ-60). The validity and reliability of DSQ were determined for Iranian samples by Heidari Nasab and colleagues [16]. In the aforementioned study, the questionnaire’s reliability was determined using test re-test methods and the Cronbach α. In their results, high Cronbach α and high test re-test correlation showed acceptable reliability in Iranian society.
In addition, to evaluate the study’s validity, the experts’ opinions on the questionnaire items and the NEO personality inventory (NEO PI-R) were also obtained. Accordingly, due to high agreement among experts on the questionnaire items and an acceptable correlation between the NEO factors and the questionnaire, its validity was confirmed for Iranian samples.
The EEQ (King & Emmons, 1990) was designed for evaluating the role of emotional expressiveness in health [9]. It includes 16 items across 3 subscales: positive emotional expressiveness (7 items), sincerity expressiveness (5 items), and negative emotional expressiveness (4 items). EEG was also scored on a Likert scale, with a completely compatible answer scored 5 and a completely opposing answer scored 1. In this questionnaire, the total score ranges from 16 to 80, and higher scores indicate greater emotional expressiveness. Validity and reliability of the questionnaire were confirmed using the internal consistency (Cronbach α: Total 68%) and re-test methods (total 79%), respectively.
The SPI was another questionnaire that we employed. It was written by Connor and colleagues in 2000 to evaluate social phobia [17]. The questionnaire contains 17 items and 3 subscales: Fear in social situations (6 items), avoiding social situations (7 items), and physiological discomfort in social situations (4 items) in which the patient is asked to scale his/her suffer during the recent week: 0 (never), 1 (low), 2 (somewhat), 3 (much), 4 (too much). The total score ranges from 0 to 68, and the questionnaire has high reliability and validity. Its reliability and internal consistency are reported to be high, 0.78-0.89 and 0.94, using the retest method and Cronbach’s α, respectively.
Statistical analyses
SPSS software, version 22 was used to analyze the data. Accordingly, statistical indices of the Mean±SD, and the t-test, were used. The t-tests and correlation coefficient (covariance) were used for calculating the relationship between demographic characteristics and defensive mechanisms or social phobia disorder. Moreover, the Pearson chi-squared test was used to calculate the relationship between demographic characteristics and emotional expressiveness.
3. Results
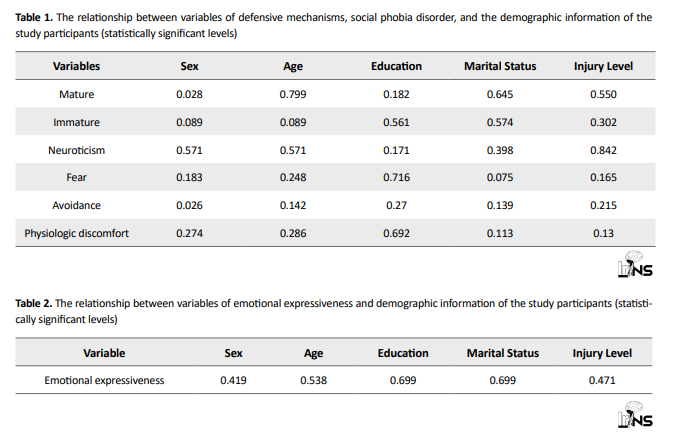
Descriptive information obtained from the questionnaires is given in Tables 1 and 2. Our findings were reported regarding the relationship between demographic characteristics (sex, age, education, and the injury level) with the study variables (defensive mechanisms, emotional expressiveness, and social phobia disorder). On the whole, there is no significant relationship between the demographic characteristics and either social phobia disorder or emotional expressiveness. However, a significant relationship was observed between mature defense styles and being single (P<0.05; Tables 1 and 2).
According to Table 3, there is a significant relationship between defensive mechanisms and emotional expressiveness. However, no significant relationship was observed between defensive mechanisms and social phobia disorder.
.PNG)
.PNG)
4. Discussion
The current study evaluated the role of defensive mechanisms on emotional expressiveness and symptoms of social phobia disorder in spinal cord-injured individuals. Our results did not reveal any significant relationship between demographic characteristics and social phobia disorder or emotional expressiveness. On the other hand, between demographic characteristics and defensive mechanisms in single participants with mature styles, a significant relationship was obtained. Notably, defensive mechanisms protect individuals against stress resulting from life’s disturbing circumstances. Adopting mature defense styles can lead to better relief, whereas immature styles can cause undesirable social consequences.
Our results demonstrated a significant relationship between defensive mechanisms and emotional expressiveness. These observations are consistent with a study by Zandi et al. [18]. They showed that adaptable and extroverted personality traits can predict the adoption of mature defensive mechanisms; nevertheless, neurotic personality traits predict the adoption of immaturemechanisms [18]. In another study, SCI patients used a sense of humor as their primary defense mechanism and rarely used immature defenses [19]. Notably, immature mechanisms are adopted primarily in the first year after the injury, as they distort reality to protect patients from discomfort. Nonetheless, over time, they adopt more mature mechanisms. Mature mechanisms do not falsify reality; instead, they teach patients how to predict stressful conditions and be better prepared to deal with them. In a cross-sectional study, the prevalence of adjustment disorders was estimated at 28% in SCI individuals, and the pattern of defensive styles was identified [20]. The most common defensive style was reported to be neurotic, and the most dominant defensive mechanism was idealization, in which the person attributes exaggeratedly positive qualities to the self. In addition, the role of demographic variables related to the injury in determining defensive mechanisms was not significant [20].
Two-dimensional structures of adaptability were observed in individuals with SCI. One dimension illustrates adaptive responses relative to nonadaptive ones, and the other demonstrates denial of the disturbances resulting from SCI. Their investigation suggests that adaptability and SCI compatibility are complex processes [21]. Similarly, it has been shown that during the adaptability process, feelings of suppression or denial gradually fade, and finally, psychological acceptance is achieved [22].Moreover, as spinal cord-injured people perceive that external factors are controlling their lives, along with their low self-confidence, feelings of helplessness, and despair, they may adopt distinct defensive styles [23]. Although it has been stated in another study that the majority of SCI patients adopt an adaptive coping style, a considerable number of patients adopt nonadaptive styles [24].
On the other hand, most SCI patients can handle their disability consequences without facing any psychological discomfort. However, the coping strategies that they adopt need to be discussed [25].
Additionally, a comparison has been done regarding the effectiveness of cognitive behavioral therapy (CBT), processing emotion regulation, and a combined intervention on anxiety sensitivity of multiple sclerosis (MS) patients. The result demonstrated the effects of CBT and processing emotion regulation in the reduction of anxiety sensitivity of the patients [26].
Additionally, the role of coping styles and personality traits in eating-disordered behaviors has been shown. The results revealed substantial correlations between eating-disordered behaviors and emotion-oriented coping, task-oriented coping, agreeableness, neuroticism, and conscientiousness personality traits. In fact, individuals develop eating-disordered behaviors as a means of encountering difficulties, resulting in an interaction between coping styles and personality traits [27].
The outcomes of the current study demonstrated no significant relationships between defensive mechanisms and social phobia disorder. Nevertheless, these results are not in line with those of Saghirzadeh et al. who found that increasing adoption of mature defensive tools enhanced self-efficacy among ischemic heart patients [13].
The social disorder can be considered a stable pattern of social phobias. Using defensive mechanisms is a measure of an individual’s resilience, helping prevent a loss of self-esteem. A person with SCI, according to the level of injury, may be able to control his/her social phobia. Although social phobia is a comprehensive disorder, it mostly manifests in childhood and adolescence. However, SCI usually occurs at an older age, and in our study, the patients ranged from young to older.
Our results demonstrate that SCI individuals showed their emotions with defensive mechanisms. Accordingly, preventive measures should be taken to help patients adopt suitable defensive mechanisms tailored to each person’s physical and mental conditions. Additionally, due to their unusual condition, the patients should be helped to express their negative emotions to minimize harm to themselves, their families, and society. To achieve this, educational workshops on emotional expressiveness and emotional control, as well as on adopting appropriate defensive mechanisms, can be held for patients. Education and guidance for individuals with SCI can significantly impact their health and lifestyle. As a result, evaluating psychological defensive mechanisms in spinal cord-injured persons is of great importance in clinics to prevent measures from being taken in individuals prone to adopting maladaptive coping behaviors.
Among the study’s restrictions, limited access to patients and the need to commute to and transport patients should be noted, which led to a lack of referrals or reduced referrals to the health centers. Moreover, this study suggests that, for a comprehensive investigation in the future, healthy individuals should also be included to provide a more accurate comparison between healthy and SCI individuals.
5. Conclusion
There is no significant relationship between defensive mechanisms and social phobia disorder in SCI individuals. However, a significant difference was obtained between defensive mechanisms and emotional expressiveness. Social phobia disorder is a constant pattern of social phobias. SCI patients probably manage their social phobia regarding the injury type and express their emotions with defensive mechanisms. As a result, preventive measures should be taken to help them adopt mature mechanisms that account for their physical and psychological conditions. Therefore, damages resulting from negative emotional expressiveness imposed on themselves, their families, and society will be managed. Appropriate training and guidance for these individuals can improve their situation. Consequently, assessing psychological defensive mechanisms to design and implement preventive actions for individuals prone to nonadaptive coping behaviors is clinically important.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committees of Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran (Code: IR.TUMS.NI.REC.1402.001).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualiation and study design: Nila Elmi Manesh and Majid Saffarinia; Data collection, data analysis, interpretation, and writing the original draft: Sima Garshasbi; Review and editing : Nila Elmi Manesh and Sima Garshasbi; Final approval: Seyed Hassan Emami-Razavi and Majid Saffarinia.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors want to thank Nahid Yarmohammadi, the chairman of the board of the Association for the Protection of People Living with Spinal Cord Disabilities, for her assistance in accessing the patients and gathering the necessary information. The authors would also like to thank all the patients who agreed to participate in their study.
References
Spinal cord injury (SCI) is defined as any damage to the spinal cord that can result from either trauma or disease. The majority of the spinal injuries result from trauma (90%). The symptoms of spinal injury depend on the severity of the injury and its location. The SCI signs include loss of sensation and control of leg and hand movements. The most severe SCI occurs when the systems regulating the functions of the intestines, the bladder, the respiratory system, the heartbeat, and blood pressure are disturbed. Most spinal cord-injured patients suffer chronic pain [1]. The World Health Organization (WHO) estimates that the global incidence of SCI is 40-80 cases in every million individuals. SCI prevalence in Iran is estimated to be virtually 40-50 cases in every million individuals [2]. Some secondary complications accompany SCI, which can be disabling and even threaten life. Among secondary complications are deep vein thrombosis (DVT), urinary system infections, muscular spasms, osteoporosis, chronic pain, and respiratory consequences [3].
SCI can result in serious hygienic, physical, and social impacts on affected patients, imposing considerable negative effects on their quality of life [4]. Along with physical consequences of SCI, it is estimated that 20-30% of the patients will experience symptoms of depression, which has a negative influence on the function and general health. Besides, SCI leads to mental situations such as anxiety, identity disturbance, and feeling lonely. Moreover, suicide, drug abuse, and separation are more frequent in these patients compared to normal persons [3]. The prevalence of depression and anxiety in SCI patients is reported as 30-40% and 20-25%, respectively [5]. One of the significant negative impacts on SCI patients is changes in life quality and its resulting psychological complications [6]. The stress as a result of SCI disability makes the patients isolated and socially detached. Consequently, the patients get depressed and feel incompetent. Nowadays, emotional health is considered one of the most important pillars of health.
Accordingly, emotional health is stated as emotional perception and the ability to cope with everyday life issues. An emotionally healthy person correctly distinguishes his emotions and expresses them in appropriate situations [7]. Emotional expressiveness is defined as an external display of emotion, regardless of its positive or negative value, whether expressed verbally or physically. People express their emotions differently. Some individuals express their emotions freely without considering the consequences, a trait called emotional expressiveness. Nevertheless, some adopt a conservative approach and do not express their emotions. In some others, inhibition of emotions leads to mental confusion and even physical problems in them, and these people suffer from emotional inhibition [7].
The emotion has 4 functions: organizing excitement, fostering self-understanding, improving coping skills, and strengthening interpersonal relationships [8]. According to King and Emmons, emotional expression does not necessarily indicate health; rather, the person’s feelings toward these expressive behaviors indicate the health. To express the emotional role of health, three emotional expression dimensions are considered: negative expression, positive expression, and sincerity expression [9]. Several studies have been conducted in this field and demonstrate a relationship between emotional expressiveness and some physical illnesses like cancer and cardiovascular diseases [7]. A positive relationship between positive emotional expression and psychological well-being was reported by Kennedy-Moore and Watson [8]. Misconception, negative attitude, and physical obstacles lead to a considerable deprivation in spinal cord-injured patients, which does not permit their active participation in society. For instance, children with SCI start school later compared to their peers and even progress more slowly at school. Likewise, people with physical disabilities make fewer social contacts and have a great tendency to loneliness and isolation compared to ordinary persons [10]. Social anxiety disorder or social phobia is a disabling disorder that can influence a considerable portion of society [11]. In fact, social phobia disorder is the most prevalent disorder in childhood and adolescence [3]. According to Rapee, social anxiety disorder includes a wide range of anxiety: No social anxiety, normal level of social anxiety, social anxiety (low level of shame), fears and social avoidances (social anxiety disorder), pervasive level of social anxiety disorder, and avoidant personality disorder [12].
Defense mechanisms are unconscious mental processes that protect against different kinds of anxiety. These mechanisms not only protect individuals against anxiety and warn about possible dangers and internal stressors but also regulate mental experiences related to painful thoughts, feelings, and emotions [13]. According to Vailnat’s hierarchical classification, defensive mechanisms are divided into 20 mechanisms in 3 defensive styles: mature defense styles, immature defense styles, and neuroticism. Mature defensive mechanisms are considered adaptive, normal, and efficient coping styles, while immature and neurotic defensive mechanisms are nonadaptive and inefficient coping styles. Notably, people adopt different defensive styles in specific situations [14].
Until now, several studies have been carried out on defensive mechanisms, emotional expression, and social anxiety disorder for different target groups who deal with chronic diseases. Nonetheless, defensive mechanisms in individuals with SCI have not been fully evaluated in Iran. The current study aims to investigate the role of defensive mechanisms on emotional expression and symptoms of social anxiety disorder in SCI patients. Eventually, we hope the findings of this investigation help SCI patients receive the necessary education and therapeutic interventions, such as emotional expression, defensive mechanisms, etc. to prevent social anxiety disorder in them.
2. Methods and Materials/Patients
The study sample
The current study, which began in April 2023 and lasted 1 year, was descriptive, correlational, and survey-based. The study population consisted of SCI patients who were referred to the medical centers of the State Welfare Organization of Tehran Province. Initially, ethical approval was obtained to conduct this study. Then, the patients were invited verbally to participate in our investigation. The sample size was determined using G*Power software, version 3.1 with a type I error (false positive) rate of 5%, a power of 80%, and a medium effect size of 0.6, yielding a sample size of 115. The inclusion criterion was adults with SCI and literacy. The exclusion criteria were failure to meet the inclusion criteria and unwillingness to participate in the study.
The questionnaires were distributed to 115 participants, and at the end, 100 were completed; 15 patients dropped out during the study. Demographic characteristics of the participants were as follows: 31 women and 69 men; 56.7% married and 40.2% single; 6.2% with undergraduate education, 57.7% with diploma education, and 32% with university education. According to the levels of SCI, 44.3% had lumbar, 36.1% cervical, and 17.5% thoracic injuries.
Study questionnaires
To collect the research findings, the defense style questionnaire (DSQ), the emotional expressiveness questionnaire (EEQ), and the social phobia inventory (SPI) were employed. DSQ was prepared by Andrews and colleagues [15]. It is scored on a Likert scale and consists of 40 questions, each assessing 20 defensive mechanisms across 3 levels: Undeveloped, developed, and neuroticism. For each defensive mechanism, the score ranges from 2 to 18. Scores >10 indicate that the person uses this mechanism. In each defensive style, a person’s average score indicates the defensive mechanism he uses; the highest score indicates the defensive style he uses. The internal reliability of this instrument has been reported to range from 0.75 to 0.85 across studies, and its factor structure has been confirmed across several versions (including DSQ-40 and DSQ-60). The validity and reliability of DSQ were determined for Iranian samples by Heidari Nasab and colleagues [16]. In the aforementioned study, the questionnaire’s reliability was determined using test re-test methods and the Cronbach α. In their results, high Cronbach α and high test re-test correlation showed acceptable reliability in Iranian society.
In addition, to evaluate the study’s validity, the experts’ opinions on the questionnaire items and the NEO personality inventory (NEO PI-R) were also obtained. Accordingly, due to high agreement among experts on the questionnaire items and an acceptable correlation between the NEO factors and the questionnaire, its validity was confirmed for Iranian samples.
The EEQ (King & Emmons, 1990) was designed for evaluating the role of emotional expressiveness in health [9]. It includes 16 items across 3 subscales: positive emotional expressiveness (7 items), sincerity expressiveness (5 items), and negative emotional expressiveness (4 items). EEG was also scored on a Likert scale, with a completely compatible answer scored 5 and a completely opposing answer scored 1. In this questionnaire, the total score ranges from 16 to 80, and higher scores indicate greater emotional expressiveness. Validity and reliability of the questionnaire were confirmed using the internal consistency (Cronbach α: Total 68%) and re-test methods (total 79%), respectively.
The SPI was another questionnaire that we employed. It was written by Connor and colleagues in 2000 to evaluate social phobia [17]. The questionnaire contains 17 items and 3 subscales: Fear in social situations (6 items), avoiding social situations (7 items), and physiological discomfort in social situations (4 items) in which the patient is asked to scale his/her suffer during the recent week: 0 (never), 1 (low), 2 (somewhat), 3 (much), 4 (too much). The total score ranges from 0 to 68, and the questionnaire has high reliability and validity. Its reliability and internal consistency are reported to be high, 0.78-0.89 and 0.94, using the retest method and Cronbach’s α, respectively.
Statistical analyses
SPSS software, version 22 was used to analyze the data. Accordingly, statistical indices of the Mean±SD, and the t-test, were used. The t-tests and correlation coefficient (covariance) were used for calculating the relationship between demographic characteristics and defensive mechanisms or social phobia disorder. Moreover, the Pearson chi-squared test was used to calculate the relationship between demographic characteristics and emotional expressiveness.
3. Results
Descriptive information obtained from the questionnaires is given in Tables 1 and 2. Our findings were reported regarding the relationship between demographic characteristics (sex, age, education, and the injury level) with the study variables (defensive mechanisms, emotional expressiveness, and social phobia disorder). On the whole, there is no significant relationship between the demographic characteristics and either social phobia disorder or emotional expressiveness. However, a significant relationship was observed between mature defense styles and being single (P<0.05; Tables 1 and 2).
According to Table 3, there is a significant relationship between defensive mechanisms and emotional expressiveness. However, no significant relationship was observed between defensive mechanisms and social phobia disorder.
4. Discussion
The current study evaluated the role of defensive mechanisms on emotional expressiveness and symptoms of social phobia disorder in spinal cord-injured individuals. Our results did not reveal any significant relationship between demographic characteristics and social phobia disorder or emotional expressiveness. On the other hand, between demographic characteristics and defensive mechanisms in single participants with mature styles, a significant relationship was obtained. Notably, defensive mechanisms protect individuals against stress resulting from life’s disturbing circumstances. Adopting mature defense styles can lead to better relief, whereas immature styles can cause undesirable social consequences.
Our results demonstrated a significant relationship between defensive mechanisms and emotional expressiveness. These observations are consistent with a study by Zandi et al. [18]. They showed that adaptable and extroverted personality traits can predict the adoption of mature defensive mechanisms; nevertheless, neurotic personality traits predict the adoption of immaturemechanisms [18]. In another study, SCI patients used a sense of humor as their primary defense mechanism and rarely used immature defenses [19]. Notably, immature mechanisms are adopted primarily in the first year after the injury, as they distort reality to protect patients from discomfort. Nonetheless, over time, they adopt more mature mechanisms. Mature mechanisms do not falsify reality; instead, they teach patients how to predict stressful conditions and be better prepared to deal with them. In a cross-sectional study, the prevalence of adjustment disorders was estimated at 28% in SCI individuals, and the pattern of defensive styles was identified [20]. The most common defensive style was reported to be neurotic, and the most dominant defensive mechanism was idealization, in which the person attributes exaggeratedly positive qualities to the self. In addition, the role of demographic variables related to the injury in determining defensive mechanisms was not significant [20].
Two-dimensional structures of adaptability were observed in individuals with SCI. One dimension illustrates adaptive responses relative to nonadaptive ones, and the other demonstrates denial of the disturbances resulting from SCI. Their investigation suggests that adaptability and SCI compatibility are complex processes [21]. Similarly, it has been shown that during the adaptability process, feelings of suppression or denial gradually fade, and finally, psychological acceptance is achieved [22].Moreover, as spinal cord-injured people perceive that external factors are controlling their lives, along with their low self-confidence, feelings of helplessness, and despair, they may adopt distinct defensive styles [23]. Although it has been stated in another study that the majority of SCI patients adopt an adaptive coping style, a considerable number of patients adopt nonadaptive styles [24].
On the other hand, most SCI patients can handle their disability consequences without facing any psychological discomfort. However, the coping strategies that they adopt need to be discussed [25].
Additionally, a comparison has been done regarding the effectiveness of cognitive behavioral therapy (CBT), processing emotion regulation, and a combined intervention on anxiety sensitivity of multiple sclerosis (MS) patients. The result demonstrated the effects of CBT and processing emotion regulation in the reduction of anxiety sensitivity of the patients [26].
Additionally, the role of coping styles and personality traits in eating-disordered behaviors has been shown. The results revealed substantial correlations between eating-disordered behaviors and emotion-oriented coping, task-oriented coping, agreeableness, neuroticism, and conscientiousness personality traits. In fact, individuals develop eating-disordered behaviors as a means of encountering difficulties, resulting in an interaction between coping styles and personality traits [27].
The outcomes of the current study demonstrated no significant relationships between defensive mechanisms and social phobia disorder. Nevertheless, these results are not in line with those of Saghirzadeh et al. who found that increasing adoption of mature defensive tools enhanced self-efficacy among ischemic heart patients [13].
The social disorder can be considered a stable pattern of social phobias. Using defensive mechanisms is a measure of an individual’s resilience, helping prevent a loss of self-esteem. A person with SCI, according to the level of injury, may be able to control his/her social phobia. Although social phobia is a comprehensive disorder, it mostly manifests in childhood and adolescence. However, SCI usually occurs at an older age, and in our study, the patients ranged from young to older.
Our results demonstrate that SCI individuals showed their emotions with defensive mechanisms. Accordingly, preventive measures should be taken to help patients adopt suitable defensive mechanisms tailored to each person’s physical and mental conditions. Additionally, due to their unusual condition, the patients should be helped to express their negative emotions to minimize harm to themselves, their families, and society. To achieve this, educational workshops on emotional expressiveness and emotional control, as well as on adopting appropriate defensive mechanisms, can be held for patients. Education and guidance for individuals with SCI can significantly impact their health and lifestyle. As a result, evaluating psychological defensive mechanisms in spinal cord-injured persons is of great importance in clinics to prevent measures from being taken in individuals prone to adopting maladaptive coping behaviors.
Among the study’s restrictions, limited access to patients and the need to commute to and transport patients should be noted, which led to a lack of referrals or reduced referrals to the health centers. Moreover, this study suggests that, for a comprehensive investigation in the future, healthy individuals should also be included to provide a more accurate comparison between healthy and SCI individuals.
5. Conclusion
There is no significant relationship between defensive mechanisms and social phobia disorder in SCI individuals. However, a significant difference was obtained between defensive mechanisms and emotional expressiveness. Social phobia disorder is a constant pattern of social phobias. SCI patients probably manage their social phobia regarding the injury type and express their emotions with defensive mechanisms. As a result, preventive measures should be taken to help them adopt mature mechanisms that account for their physical and psychological conditions. Therefore, damages resulting from negative emotional expressiveness imposed on themselves, their families, and society will be managed. Appropriate training and guidance for these individuals can improve their situation. Consequently, assessing psychological defensive mechanisms to design and implement preventive actions for individuals prone to nonadaptive coping behaviors is clinically important.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committees of Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran (Code: IR.TUMS.NI.REC.1402.001).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualiation and study design: Nila Elmi Manesh and Majid Saffarinia; Data collection, data analysis, interpretation, and writing the original draft: Sima Garshasbi; Review and editing : Nila Elmi Manesh and Sima Garshasbi; Final approval: Seyed Hassan Emami-Razavi and Majid Saffarinia.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors want to thank Nahid Yarmohammadi, the chairman of the board of the Association for the Protection of People Living with Spinal Cord Disabilities, for her assistance in accessing the patients and gathering the necessary information. The authors would also like to thank all the patients who agreed to participate in their study.
References
- Krahn GL. WHO world report on disability: A review. Disability and Health Journal. 2011; 4(3):141-2. [DOI:10.1016/j.dhjo.2011.05.001] [PMID]
- Heller MM, Wong JW, Nguyen TV, Lee ES, Bhutani T, Menter A, et al. Quality-of-life instruments: Evaluation of the impact of psoriasis on patients. Dermatologic Clinics. 2012; 30(2):281-91. [DOI:10.1016/j.det.2011.11.006] [PMID]
- Dadsetan P, Anari A, Saleh Sedghpour B. [Social anxiety disorders and drama-therapy (Persian)]. Journal of Developmental Psychology. 2008; 4(14):115-23. [Link]
- Zeqeibi Ghannad S, Fateminik T, Alipoor S. The role of sleep quality, social support and fatigue on daily life self-efficacy in people with spinal cord injury. Iranian Journal of Psychiatric Nursing. 2017; 5(5):26-33. [DOI:10.21859/ijpn-05054]
- Rahmani RA, Hosseini SA, Haghgoo H, Khankeh HR, Ray G. [Aspects related to resilience in people with spinal cord injury (Persian)]. Archive of Rehabilitation. 2017; 17(4):350-9. [DOI:10.21859/jrehab-1704350]
- Khazaeli K, Hoseini E, Nasir AH, Amarloui M, Ganji MK. [Relationship between level of injury and quality of life in spinal cord injury (SCI) patients (Persian)]. Payesh. 2019;18(1):45-51. [Link]
- Mahdavi E, Manshaee G. [Comparing alexithymia and emotional expressiveness in patients with coronary heart disease and healthy people (Persian)]. KAUMS Journal. 2016; 20(3):260-6. [Link]
- Kennedy-Moore E, Watson JC. Expressing emotion: Myths, realities, and therapeutic strategies. New York: Guilford Press; 2001. [Link]
- King LA, Emmons RA. Conflict over emotional expression: Psychological and physical correlates. Journal of Personality and Social Psychology. 1990; 58(5):864. [DOI:10.1037/0022-3514.58.5.864] [PMID]
- Hasanzadeh Pashang S, Zare H, Alipor A. The efficacy of stress inculation training (SIT) on resilience, anxiety, depression and stress among spinal cord injury (SCI) patients. Journal of Jahrom University of Medical Sciences. 2012; 10(3):15-26. [DOI:10.29252/jmj.10.3.15]
- Sararoodi B, Omidi A, Mohammadi Z. [Etiological models of social anxiety disorder (Persian)]. Journal of Research in Behavioural Sciences. 2014;11(1):68-80. [Link]
- Rapee RM, Spence SH. The etiology of social phobia: Empirical evidence and an initial model. Clinical Psychology Review. 2004; 24(7):737-67. [DOI:10.1016/j.cpr.2004.06.004] [PMID]
- Saghirzadeh M, Sadeghi N, Azarbarzin M. The relationship between defense mechanisms and self-efficacy in ischemic heart patients at Feiz Hospital of Esfahan in 2017. Avicenna Journal of Nursing and Midwifery Care. 2019; 27(3):170-7. [DOI:10.30699/ajnmc.27.3.170]
- Gharibi H, Rostami C, Mohamadian Sharif K, Monqi T. [Prediction of defense mechanisms based on the quality of life and perceived social-emotional support in married women (Persian)]. Journal of Health and Care. 2016; 18(1):73-83. [Link]
- Andrews G, Singh M, Bond M. The defense style questionnaire. Journal of Nervous and Mental Disease. 1993. [DOI:10.1037/t20765-000]
- Heidari Nasab L, Mansouri M, Azadfallah P, Shaieeri M. [Validity and reliability of defens style questionaire (DSQ-40) in Iranian samples (Persian)]. Clinical Psychology and Personality. 2007; 5(1):11-27. [Link]
- Connor KM, Davidson JR, Churchill LE, Sherwood A, Weisler RH, Foa E. Psychometric properties of the Social Phobia Inventory (SPIN): New self-rating scale. The British Journal of Psychiatry. 2000; 176(4):379-86. [DOI:10.1192/bjp.176.4.379] [PMID]
- Zandi S, Shahabinejad Z, Borhan A. Predicting defense mechanisms based on big five personality traitsamong university students. Zanko Journal of Medical Sciences. 2017; 18(56):1. [Link]
- Shakeri J, Yazdanshenas Ghazwin M, Rakizadeh E, Moshari A, Sharbatdaralaei H, Latifi S, et al. Do spinal cord-injured individuals with stronger sense of coherence use different psychological defense styles? Spinal Cord. 2016; 54(10):843-8. [DOI:10.1038/sc.2015.213] [PMID]
- Yazdanshenas Ghazwin M, Tavakoli SAH, Latifi S, Saberi H, Derakhshanrad N, Yekaninejad MS, et al. Psychological defense mechanisms among individuals with SCI with adjustment disorder. The Journal of Spinal Cord Medicine. 2017; 40(5):538-47. [DOI:10.1080/10790268.2016.1140389] [PMID]
- Livneh H, Martz E. Psychosocial adaptation to spinal cord injury: A dimensional perspective. Psychological Reports. 2005; 97(2):577-86. [DOI:10.2466/PR0.97.6.577-586] [PMID]
- Fukunishi I, Koyama I, Tobimatsu H. Psychological acceptance and alexithymia in spinal cord injury patients. Psychological Reports. 1995; 76(2):475-81. [DOI:10.2466/pr0.1995.76.2.475] [PMID]
- Craig AR, Hancock K, Chang E. The influence of spinal cord injury on coping styles and self-perceptions two years after the injury. Australian and New Zealand Journal of Psychiatry. 1994; 28(2):307-12. [DOI:10.1080/00048679409075644] [PMID]
- Hancock K, Craig A, Tennant C, Chang E. The influence of spinal cord injury on coping styles and self-perceptions: A controlled study. Australian and New Zealand Journal of Psychiatry. 1993; 27(3):450-6. [DOI:10.3109/00048679309075802] [PMID]
- Pollard C, Kennedy P. A longitudinal analysis of emotional impact, coping strategies and post-traumatic psychological growth following spinal cord injury: A 10-year review. British Journal of Health Psychology. 2007; 12(3):347-62. [DOI:10.1348/135910707X197046] [PMID]
- Niknam M. Hatami M, Mohammad N. Comparing the efficacy of cognitive-behavioral therapy and processingemotion regulation on anxiety sensitivity of patients with multiple sclerosis. Journal of Health Psychology. 2021; 10(37):109-26. [Link]
- Kachuei M, Fathi Ashtiani A, Allahyari A. The role of coping styles and personality traits in eating-disordered behaviors. Quarterly Journal of Health Psychology. 2015; 4(13):63-72. [Link]
Type of Study: Clinical Trial |
Subject:
Spine
Send email to the article author
| Rights and Permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
