Wed, Jun 24, 2026
Volume 11 - Continuous Publishing
Iran J Neurosurg 2025, 11 - Continuous Publishing: 0-0 |
Back to browse issues page
Ethics code: IR.GUMS.REC.1403.146
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mardvar A, Reihanian Z, Jafari S, Modaenama M, Yazdanipour M, Torkashvand M et al . Comparative Outcomes of Combined Spinal-general Anesthesia versus General Anesthesia in Lumbar Spine Fusion Surgery. Iran J Neurosurg 2025; 11 : 23
URL: http://irjns.org/article-1-505-en.html
URL: http://irjns.org/article-1-505-en.html
Afshin Mardvar *1 

 , Zoheir Reihanian1 , Seifollah Jafari1 , Morteza Modaenama2 , Mohammadali Yazdanipour3 , Mahdieh Torkashvand4 , Ali Ashraf5
, Zoheir Reihanian1 , Seifollah Jafari1 , Morteza Modaenama2 , Mohammadali Yazdanipour3 , Mahdieh Torkashvand4 , Ali Ashraf5
, Zoheir Reihanian1 , Seifollah Jafari1 , Morteza Modaenama2 , Mohammadali Yazdanipour3 , Mahdieh Torkashvand4 , Ali Ashraf5
1- Department of Neurosurgery, School of Medicine, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran. & Road Trauma Research Center, Trauma Institute, Guilan University of Medical Sciences, Rasht, Iran
2- Department of Neurosurgery, School of Medicine, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran.
3- Neuroscience Research Center, Trauma Institute, Guilan University of Medical Sciences, Rasht, Iran.
4- Poursina Clinical Research Development Unit, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran.
5- Poursina Clinical Research Development Unit, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran. & Department of Anesthesiology, School of Medicine, , Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran
2- Department of Neurosurgery, School of Medicine, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran.
3- Neuroscience Research Center, Trauma Institute, Guilan University of Medical Sciences, Rasht, Iran.
4- Poursina Clinical Research Development Unit, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran.
5- Poursina Clinical Research Development Unit, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran. & Department of Anesthesiology, School of Medicine, , Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran
Keywords: Lumbar spine, Fusion surgery, Postoperative pain, General anesthesia, Spinal anesthesia Hemodynamic
Full Text [PDF 1511 kb]
(267 Downloads)
| Abstract (HTML) (591 Views)
Full Text: (107 Views)
1. Introduction
Lumbar spinal fusion (LSF) is a surgical procedure that fuses two or more lower vertebrae to stabilize the spine and protect the cauda equina and nerve roots. It is indicated in situations, such as vertebral fractures, infections, or tumors, with possible benefits in degenerative disease and spinal stenosis [1]. It is one of the most commonly performed procedures in spine surgery and is the treatment of choice for some degenerative spinal pathologies. Surgery on the lumbar spine for degenerative conditions alleviates pain and disability while improving overall function. Therefore, LSF is a highly effective intervention for various spinal disorders [2-4]. Instrumented spine surgeries are expected to continue increasing due to the ageing population [5, 6]. Despite the growing number of instrumented spine surgeries and the need to analyze complex interventions, there is a significant lack of published research on this topic. Most current studies primarily focus on patients’ experiences and feelings, while insights from healthcare providers remain limited [7-10]. Assessing and enhancing the efficiency of these procedures, while ensuring patient satisfaction, is critically important. Recent debates asserting the influence of primary anesthesia methods on outcomes after spine surgery emphasize the need for further research and analysis to identify best practices that improve patient outcomes and experiences [11, 12].
General anesthesia (GA) has traditionally been the accepted method for lumbar spine surgical procedures. There used to be significant differences in operating times and blood loss, as well as in the degree of invasiveness of these procedures, making it mandatory to resort to GA when adequate hemodynamic control, resuscitation, and patient comfort were required. The advancement of lumbar spinal procedures has embraced the approach of standardized minimally invasive procedures to assure less morbidity and less time for surgery. Therefore, there has been increasing interest in alternatives to GA. One such method is spinal anesthesia (SA), which typically involves the intrathecal injection of a mixture of sodium channel blockers and opioids. The surge of interest in SA as an alternative to GA has occurred recently. Both GA and SA are considered safe and efficacious for lumbar spine surgical procedures [13-15]. Several studies have indicated that SA could be a safe alternative to GA in adults undergoing lumbar decompression procedures [16-21]. Additionally, it is suggested that regional anesthesia (RA) provides greater comfort and relaxation of the erector spinae muscles, lowers blood pressure, and provides postoperative pain relief in combination with GA, compared to GA alone. Anesthetic synergy resulting from combining GA with the erector spinae plane block could thus provide an alternative to GA and improve surgeons’ working conditions [22].
At present, considering that both GA and SA possess distinct advantages and disadvantages [23], which may impact pre- and post-operative results differently, in conjunction with the absence of clear evidence regarding the impact of adding SA to GA on performing GA alone during lumbar spine fusion surgery, it is critical to conduct a study comparing these two approaches. Thus, this study sought to evaluate the pre- and postoperative outcomes of combined spinal and GA compared with GA alone in lumbar spine fusion surgery.
2. Materials and Methods
This single-blind clinical trial was conducted at a hospital in northern Iran. The study was approved by the University of Medical Sciences Ethics Committee, and the study protocol was registered with the Iranian Registry of Clinical Trials. Patients who were candidates for spinal fusion surgery were selected using convenience sampling. After providing a comprehensive explanation of the available anesthesia methods, informed consent was obtained from all participants.
Participants
Participants were selected from candidates aged 18-65 years who were scheduled for spine fusion surgeries and had an American Society of Anesthesiologists (ASA) classification of I or II. Individuals were excluded from the study if they had an ASA classification higher than class II, blood coagulation disorders, local infections, or any relative or absolute contraindications for SA. Additionally, patients who did not provide consent to participate were also excluded from the study.
Interventions
An anesthesiologist administered anesthesia to all patients. Each patient was positioned supine on the operating room bed, and standard monitoring was established, including non-invasive blood pressure measurement, pulse oximetry, and heart rate monitoring. Hydration was initiated using normal saline. After preoxygenating the patient with 100% oxygen, anesthesia induction was initiated.
In cases where only GA was used, premedication consisted of an administration of fentanyl and midazolam. This was followed by anesthesia induction using propofol at a dosage of 2-2.5 mg/kg body weight and intravenous atracurium at a dosage of 0.5 mg/kg body weight.
For the combined GSA method, after induction using the same technique, the patient was placed in a lateral position. A 25-gauge quincke needle was then used to administer bupivacaine at a dosage of 0.2 mg/kg body weight. At the end of the procedure, to reverse the effects of the muscle relaxant, atropine was administered (0.02 mg/kg) and neostigmine (0.04 mg/kg). The patient was then transferred to the recovery area.
Outcomes
Outcomes were assessed by a neurosurgery resident blinded to the intervention assignment. The primary outcome was hemodynamic changes before and after the procedure, evaluated at several key points: Patient entry into the operating room, after intubation, at the start and end of surgery, after anesthesia (upon transfer to the recovery unit), and upon discharge from recovery.
The secondary outcome focused on pain intensity before and after the procedure, utilizing a 10 cm visual analogue scale (VAS), with 0 indicating no pain and 10 indicating the most severe pain experienced by the patient [24].
All patients were monitored for side effects, including postoperative nausea, vomiting, and shivering. Vital signs, including arterial oxygen saturation (SpO2), were continuously monitored. Non-invasive oxygen supplementation was provided via a face mask (at a flow rate of 3 L/min) if SpO2 fell below 96%.
Before induction of anesthesia, the patient’s vital signs—specifically systolic and diastolic blood pressure, heart rate, and SpO2—were recorded. These measurements were also taken during the operation and recovery phases. In this study, intraoperative blood loss and total doses of propofol and midazolam were documented as primary variables. Additionally, secondary variables included the time from patient entry into the operating room to the start of surgery, the duration of surgery, and the time from the end of surgery to the patient’s discharge from recovery.
Sample size
The required sample size for this study was calculated based on the findings of Sadrolsadat et al. [25] and focused on comparing hemodynamic changes, particularly blood pressure, between two groups. In their study, hypotension during anesthesia was reported in 12% and 48% of patients in the GA group and SA groups, respectively. Utilizing a significance level of 5% and a power of 80%, with an allocation ratio of 1:1, we determined that a total sample size of 44 participants (22 per group) would be adequate to detect a clinically significant difference between the two groups. To account for a potential 10% dropout rate, we increased the sample size to 48 participants (24 per group).
Randomization and blinding
The randomization sequence was conducted using Sealed Envelopes to assign participants to two groups with a 1:1 allocation ratio, utilizing random blocks with a block size of four. The two groups consisted of a combination of GSA (n=24) and GA (n=24). The allocation process was concealed, and on the day of surgery, after confirming eligibility, a research nurse communicated the group assignment to the anesthesiologist. The participants were blinded to their treatment assignments (Figure 1).
.PNG)
Statistical analysis
IBM SPSS software, version 25 (SPSS Inc., Chicago, IL, USA) was utilized for data management and statistical analysis. Descriptive statistics, including mean, standard deviation, median, interquartile range, frequency, and percentages, were calculated for scale and categorical variables, respectively. The distribution of variables was assessed using the Shapiro-Wilk test. Continuous variables between two groups were compared using either Student’s t-test or the Mann-Whitney U test, as appropriate. Within-group comparisons were performed using the Wilcoxon signed-rank test. To compare categorical variables, the Pearson chi-square test and Fisher’s exact test were employed. A repeated-measures analysis of variance (ANOVA) was conducted to examine the effects of anesthesia type (GSA and GA) on systolic, diastolic, and mean arterial pressure (MAP) at various operative times. The level of statistical significance was set at P<0.05, and all tests were two-sided.
3. Results
This clinical trial comprised 45 patients in the study sample. GSA was used in 22 patients, and GA in 23 patients. Table 1 summarizes the baseline characteristics of the study population stratified by anesthesia type. The proportion of male patients and the ASA score were similar between the two groups. No statistically significant differences were observed between the GSA and GA groups in terms of age, weight, addiction, and general medical history (Table 1).
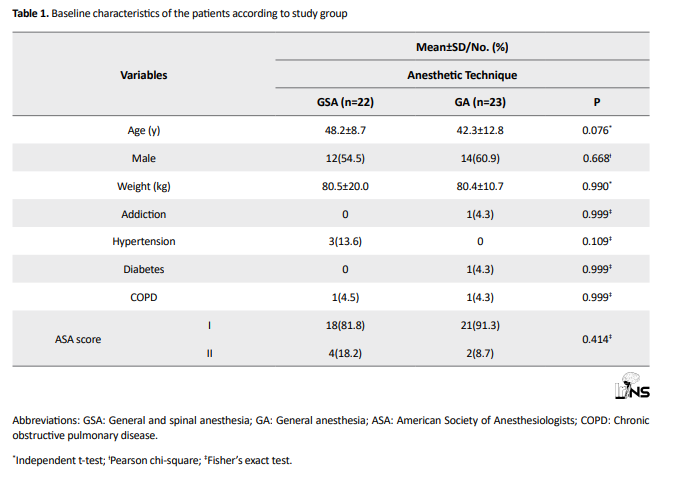
Table 2 summarizes the characteristics of the procedure and anesthesia based on the anesthesia technique used. Among the factors analyzed, only the operative time for the two techniques showed a statistically significant difference (P=0.048). The operative time was shorter with the combined anesthesia technique compared to GA. Also, no statistically significant difference was observed between the two anesthesia methods for amount of bleeding, packed cell volume, nausea/vomiting, and shivering.
.PNG)
Table 3 compares heart rate, blood SpO2, pain intensity, and hemoglobin levels at baseline and post-surgery in the two groups. The mean postoperative heart rate was significantly lower in the GSA compared to the GA (72.9±8.2 vs 81.5±11.5, P=0.007). No statistically significant differences in heart rate were found in the within-group comparisons. No statistically significant difference in mean pre- and postoperative O2Sat was observed between the two anesthesia techniques or within each technique. In both methods, postoperative pain was significantly reduced compared to preoperative levels (P<0.001). The mean postoperative pain in the GSA was significantly lower than in the GA (2.6±1.9 vs 3.9±1.8, P=0.005). No statistically significant difference in hemoglobin levels was observed before and after surgery between the two groups. However, for both methods, hemoglobin levels decreased significantly after surgery compared to before (P<0.001).

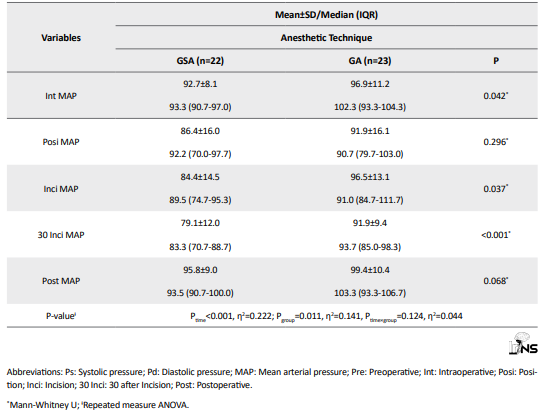
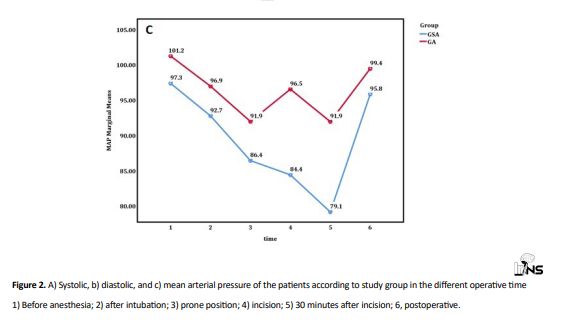
Additionally, the repeated-measures ANOVA revealed significant main effects of groups and time on systolic (Ptime<0.001; Pgroup=0.005), diastolic (Ptime<0.001; Pgroup=0.049), and MAP (Ptime<0.001; Pgroup=0.011). However, no significant interaction between the group and time was observed (Table 4 and Figure 2). As shown in Table 4, the GSA group consistently exhibited lower blood pressure compared to the GA group at all-time points. This finding indicates that GSA was consistently superior to GA in terms of blood pressure throughout the observation period.
.PNG)
Capture.PNG)
.PNG)
4. Discussion
The desired anesthetic technique should have a prompt onset and reversal of effects. It should also maintain stable hemodynamics throughout the procedure without increasing the need for blood transfusion. Finally, an ideal anesthetic should shorten recovery room time while serving as an agent against postoperative pain, nausea, and vomiting, or as a supplement to analgesics [16]. Combining two anesthetic techniques, considering the proposed benefits and drawbacks of the other, is not new [26]. Therefore, this randomized clinical trial compared perioperative and postoperative parameters in 45 patients undergoing GA versus combined spinal and GA during LSF surgery. These results have significant implications for the differences in the effects of both anesthetic techniques on operative time, cardiovascular stability, postoperative analgesia, and hemodynamic parameters.
A standout finding was the significant decrease in operative time in the combined spinal and GA group compared with the GA alone group (128.6±47.0 vs 160.9±57.3 minutes, P=0.048). This implies that the additional use of SA facilitates more efficient surgical procedures. This decrease is associated with improved hemodynamic stability, less intraoperative blood loss, and a better surgical field for the surgeon, enabling a more efficient surgical process. One study found no statistically significant difference between the SA and GA groups about operative time [27]; however, the literature on combined spinal and GA indicates an association between its use and a decrease in surgery duration compared with GA alone, particularly in lumbar spine surgeries. This decrease may be attributed to improved hemodynamic stability, decreased intraoperative blood loss, and improved surgical field conditions, which make for a more efficient surgical process [16]. Induced hypotension during spine surgery offers the added benefits of reduced blood loss and the requirement for blood transfusion [28], better operating conditions, and shorter surgical time. Combined spinal and GA can greatly reduce the actual operating time compared to GA alone. This is chiefly due to better hemodynamic stability, decreased intraoperative blood loss, and improved surgical conditions. Hence, the results favor the application of combined spinal and GA as a safe and effective anesthetic technique for specific surgical procedures. Additionally, considering the equalization of preoperative preparation time between the groups in our study, with both groups having a median preservation time of 30 minutes, the variation in operative time was seemingly independent of any potential pre-surgical delay and was accounted for by the anesthetic technique employed.
Heart rate, a significant indicator of the autonomic and hemodynamic responses to surgical stress, showed significant differences between groups postoperatively. Baseline heart rates were similar in both groups; however, the combined spinal-GA group had a lower median postoperative heart rate (73 beats per minute) compared to the GA group (83 beats per minute), and this difference was statistically significant (P=0.007). More importantly, no significant difference was observed between the groups immediately following intubation or during surgery, suggesting that the SA-based heart rate stability benefits were most evident only during the postoperative phase. Research has shown that patients who have undergone combined spinal and GA might have more stable and acceptable heart rate levels during surgery compared with patients who would receive GA alone. For example, a randomized trial for laparoscopic hysterectomy revealed better hemodynamic stability throughout the surgical procedure, including heart rate, in the combined spinal-GA group versus the GA group alone [26].
In a study focusing on patients undergoing coronary artery bypass surgery (CABG), those who received combined spinal-GA maintained a comparatively stable heart rate compared to those who received only GA. The mean heart rate was significantly improved in the combined group, suggesting better hemodynamic stability throughout the surgical procedure [29]. With SA, hypotension and bradycardia can occur due to sympathetic blockade, especially with higher block levels or in more susceptible individuals [30-32]. Hence, the combined technique may reduce the need for interventional drugs, such as beta-blockers or vasopressors to modulate heart rate changes compared to GA. The various hemodynamic benefits of combined spinal and GA are further emphasized by the alterations noted in the systolic, diastolic, and MAP during the operative phases. At maximal surgical interventions, such as incision (112 vs 127 mmHg, P<0.001) and 30 minutes post-incision (105 vs 118 mmHg, P<0.001), systolic pressure was significantly lower in the combined spinal and GA group.
Likewise, MAP was lower in the GSA group at the time of incision and thereafter at measured intervals (P=0.037, <0.001). One study showed that when SA is supplemented with GA, the sympathectomy induced by SA may counteract increases in systemic vascular resistance, thereby targeting the elevated MAP [26]. While concerns regarding hypotension generated by spinal anesthetics have been raised by some practitioners [33-35], no significant hypotension (defined as a decrease in MAP of more than 20%) was observed in our combined spinal and GA group (P=0.885), thus reinforcing that it is a safe technique when well managed.
Another area of benefit identified has been postoperative pain management, in which combined spinal and GA has shown superiority. The postoperative VAS scores of the combined spinal and GA group were significantly lower than those of the GA group (median 3.0 vs 4.0, P=0.005). Several authors have reported that combined spinal and GA provides better postoperative analgesia than GA alone. For instance, in abdominal hysterectomy, patients with combined spinal and GA had lower pain scores and required fewer postoperative analgesics than those with GA alone [36]. Similarly, in robotic sacrocervicopexy, patients anesthetized with a combination of spinal and GA reported significantly lower pain scores and less analgesic intake during the immediate postoperative period. Pain and analgesic use within the first 24 hours after robotic gynecologic surgery was significantly lower when GSA was used compared to GA alone.
A considerably higher number of GA patients requested additional analgesic medications when they reached the recovery unit, compared to a few patients who underwent combined anesthesia. The lower reported pain levels in the study group may be associated with the analgesia provided by intrathecal anesthesia [37]. This decrease in opioid consumption is crucial to prevent opioid-associated side effects and fast-tracking recovery. One study indicated that adding spinal or regional blocks to GA markedly reduces intraoperative and postoperative opioid requirements. During breast surgery, patients receiving regional block (Pecs II) plus GA consumed fewer opioids intra- and postoperatively and had lower pain scores for up to 24 hours after surgery [38]. The repeated-measures analysis of pain scores over time showed a significant group effect and a group-by-time interaction, indicating that the analgesic benefit of SA persisted and was consistent across time points.
The recovery time in the post-anesthesia care unit did not differ significantly between groups, with median times of 27.5 minutes and 30 minutes (P=0.474). This suggests that the benefits of GSA regarding operative time and pain management do not necessarily lead to a faster, immediate recovery.
The lower hemoglobin levels after surgery in both groups correlated well with the expected surgical blood loss (P<0.001). Thus it is unsurprising that perioperative bleeding was unrelated to the anesthesia method of choice, as the bleeding volumes and requirements for transfusion did not differ significantly between groups. It is reassuring in the face of concerns that regional anesthesia (RA) would increase bleeding due to vasodilation caused by sympathectomy [39]. In other words, we believe that when good surgical techniques are used, carefully selected patients can undergo combined GSA without hemostatic risk.
Despite these promising results, some disadvantages deserve attention. The small sample size (n=45) limits the generalizability of the findings, and the single-center design may have reduced variability in surgical techniques and patient demographics. While the baseline characteristics were statistically comparable between the groups, unmeasured confounders, such as intraoperative fluid management, anesthesiologists’ experience, and postoperative analgesic protocols, may influence outcomes. Larger multicenter randomized trials stratified by type of surgery and with longer follow-up periods should be conducted in the future to confirm and further build on these findings.
5. Conclusion
In conclusion, evidence from this clinical trial indicates that combined GSA provides more definitive benefits over GA alone in patients undergoing LSF surgery. Such benefits include shorter operative durations, improved postoperative heart rate regulation, more consistent intraoperative blood pressure, and better pain control in the immediate postoperative period. These advantages favor the use of SA adjuncts in appropriate surgical groups to maintain perioperative hemodynamic stability with comfort, without compromising recovery duration or increasing the risk of bleeding. These results are of great importance in guiding anesthesia practices to optimize patient outcomes and reduce perioperative risks.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Guilan University of Medical Sciences, Rasht, Iran (Code: IR.GUMS.REC.1403.146) and conducted by the Code of Ethics of the World Medical Association (Declaration of Helsinki). The study protocol was approved by the Iranian Registry of Clinical Trials (IRCT), Tehran, Iran (Code: IRCT20140310016917N11). Informed consent was obtained from all participants before their inclusion in the study.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conception and study design: Afshin Mardvar, Ali Ashraf, Zoheir Reihanian and Mahdie Torkashvand; Data collection: Afshin Mardvar, Ali Ashraf, Zoheir Reihanian, Seifollah Jafari and Morteza Modaenama; Data analysis and interpretation: Ali Ashraf and Mohammadali Yazdanipour; Drafting the article: Afshin Mardvar, Ali Ashraf and Mohammadali Yazdanipour; Critical revision of the article: Ali Ashraf, Zoheir Reihanian and Morteza Modaenama; Final Approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors acknowledge the assistance of Poursina Clinical Research Development Unit.
References
Lumbar spinal fusion (LSF) is a surgical procedure that fuses two or more lower vertebrae to stabilize the spine and protect the cauda equina and nerve roots. It is indicated in situations, such as vertebral fractures, infections, or tumors, with possible benefits in degenerative disease and spinal stenosis [1]. It is one of the most commonly performed procedures in spine surgery and is the treatment of choice for some degenerative spinal pathologies. Surgery on the lumbar spine for degenerative conditions alleviates pain and disability while improving overall function. Therefore, LSF is a highly effective intervention for various spinal disorders [2-4]. Instrumented spine surgeries are expected to continue increasing due to the ageing population [5, 6]. Despite the growing number of instrumented spine surgeries and the need to analyze complex interventions, there is a significant lack of published research on this topic. Most current studies primarily focus on patients’ experiences and feelings, while insights from healthcare providers remain limited [7-10]. Assessing and enhancing the efficiency of these procedures, while ensuring patient satisfaction, is critically important. Recent debates asserting the influence of primary anesthesia methods on outcomes after spine surgery emphasize the need for further research and analysis to identify best practices that improve patient outcomes and experiences [11, 12].
General anesthesia (GA) has traditionally been the accepted method for lumbar spine surgical procedures. There used to be significant differences in operating times and blood loss, as well as in the degree of invasiveness of these procedures, making it mandatory to resort to GA when adequate hemodynamic control, resuscitation, and patient comfort were required. The advancement of lumbar spinal procedures has embraced the approach of standardized minimally invasive procedures to assure less morbidity and less time for surgery. Therefore, there has been increasing interest in alternatives to GA. One such method is spinal anesthesia (SA), which typically involves the intrathecal injection of a mixture of sodium channel blockers and opioids. The surge of interest in SA as an alternative to GA has occurred recently. Both GA and SA are considered safe and efficacious for lumbar spine surgical procedures [13-15]. Several studies have indicated that SA could be a safe alternative to GA in adults undergoing lumbar decompression procedures [16-21]. Additionally, it is suggested that regional anesthesia (RA) provides greater comfort and relaxation of the erector spinae muscles, lowers blood pressure, and provides postoperative pain relief in combination with GA, compared to GA alone. Anesthetic synergy resulting from combining GA with the erector spinae plane block could thus provide an alternative to GA and improve surgeons’ working conditions [22].
At present, considering that both GA and SA possess distinct advantages and disadvantages [23], which may impact pre- and post-operative results differently, in conjunction with the absence of clear evidence regarding the impact of adding SA to GA on performing GA alone during lumbar spine fusion surgery, it is critical to conduct a study comparing these two approaches. Thus, this study sought to evaluate the pre- and postoperative outcomes of combined spinal and GA compared with GA alone in lumbar spine fusion surgery.
2. Materials and Methods
This single-blind clinical trial was conducted at a hospital in northern Iran. The study was approved by the University of Medical Sciences Ethics Committee, and the study protocol was registered with the Iranian Registry of Clinical Trials. Patients who were candidates for spinal fusion surgery were selected using convenience sampling. After providing a comprehensive explanation of the available anesthesia methods, informed consent was obtained from all participants.
Participants
Participants were selected from candidates aged 18-65 years who were scheduled for spine fusion surgeries and had an American Society of Anesthesiologists (ASA) classification of I or II. Individuals were excluded from the study if they had an ASA classification higher than class II, blood coagulation disorders, local infections, or any relative or absolute contraindications for SA. Additionally, patients who did not provide consent to participate were also excluded from the study.
Interventions
An anesthesiologist administered anesthesia to all patients. Each patient was positioned supine on the operating room bed, and standard monitoring was established, including non-invasive blood pressure measurement, pulse oximetry, and heart rate monitoring. Hydration was initiated using normal saline. After preoxygenating the patient with 100% oxygen, anesthesia induction was initiated.
In cases where only GA was used, premedication consisted of an administration of fentanyl and midazolam. This was followed by anesthesia induction using propofol at a dosage of 2-2.5 mg/kg body weight and intravenous atracurium at a dosage of 0.5 mg/kg body weight.
For the combined GSA method, after induction using the same technique, the patient was placed in a lateral position. A 25-gauge quincke needle was then used to administer bupivacaine at a dosage of 0.2 mg/kg body weight. At the end of the procedure, to reverse the effects of the muscle relaxant, atropine was administered (0.02 mg/kg) and neostigmine (0.04 mg/kg). The patient was then transferred to the recovery area.
Outcomes
Outcomes were assessed by a neurosurgery resident blinded to the intervention assignment. The primary outcome was hemodynamic changes before and after the procedure, evaluated at several key points: Patient entry into the operating room, after intubation, at the start and end of surgery, after anesthesia (upon transfer to the recovery unit), and upon discharge from recovery.
The secondary outcome focused on pain intensity before and after the procedure, utilizing a 10 cm visual analogue scale (VAS), with 0 indicating no pain and 10 indicating the most severe pain experienced by the patient [24].
All patients were monitored for side effects, including postoperative nausea, vomiting, and shivering. Vital signs, including arterial oxygen saturation (SpO2), were continuously monitored. Non-invasive oxygen supplementation was provided via a face mask (at a flow rate of 3 L/min) if SpO2 fell below 96%.
Before induction of anesthesia, the patient’s vital signs—specifically systolic and diastolic blood pressure, heart rate, and SpO2—were recorded. These measurements were also taken during the operation and recovery phases. In this study, intraoperative blood loss and total doses of propofol and midazolam were documented as primary variables. Additionally, secondary variables included the time from patient entry into the operating room to the start of surgery, the duration of surgery, and the time from the end of surgery to the patient’s discharge from recovery.
Sample size
The required sample size for this study was calculated based on the findings of Sadrolsadat et al. [25] and focused on comparing hemodynamic changes, particularly blood pressure, between two groups. In their study, hypotension during anesthesia was reported in 12% and 48% of patients in the GA group and SA groups, respectively. Utilizing a significance level of 5% and a power of 80%, with an allocation ratio of 1:1, we determined that a total sample size of 44 participants (22 per group) would be adequate to detect a clinically significant difference between the two groups. To account for a potential 10% dropout rate, we increased the sample size to 48 participants (24 per group).
Randomization and blinding
The randomization sequence was conducted using Sealed Envelopes to assign participants to two groups with a 1:1 allocation ratio, utilizing random blocks with a block size of four. The two groups consisted of a combination of GSA (n=24) and GA (n=24). The allocation process was concealed, and on the day of surgery, after confirming eligibility, a research nurse communicated the group assignment to the anesthesiologist. The participants were blinded to their treatment assignments (Figure 1).
Statistical analysis
IBM SPSS software, version 25 (SPSS Inc., Chicago, IL, USA) was utilized for data management and statistical analysis. Descriptive statistics, including mean, standard deviation, median, interquartile range, frequency, and percentages, were calculated for scale and categorical variables, respectively. The distribution of variables was assessed using the Shapiro-Wilk test. Continuous variables between two groups were compared using either Student’s t-test or the Mann-Whitney U test, as appropriate. Within-group comparisons were performed using the Wilcoxon signed-rank test. To compare categorical variables, the Pearson chi-square test and Fisher’s exact test were employed. A repeated-measures analysis of variance (ANOVA) was conducted to examine the effects of anesthesia type (GSA and GA) on systolic, diastolic, and mean arterial pressure (MAP) at various operative times. The level of statistical significance was set at P<0.05, and all tests were two-sided.
3. Results
This clinical trial comprised 45 patients in the study sample. GSA was used in 22 patients, and GA in 23 patients. Table 1 summarizes the baseline characteristics of the study population stratified by anesthesia type. The proportion of male patients and the ASA score were similar between the two groups. No statistically significant differences were observed between the GSA and GA groups in terms of age, weight, addiction, and general medical history (Table 1).
Table 2 summarizes the characteristics of the procedure and anesthesia based on the anesthesia technique used. Among the factors analyzed, only the operative time for the two techniques showed a statistically significant difference (P=0.048). The operative time was shorter with the combined anesthesia technique compared to GA. Also, no statistically significant difference was observed between the two anesthesia methods for amount of bleeding, packed cell volume, nausea/vomiting, and shivering.
Table 3 compares heart rate, blood SpO2, pain intensity, and hemoglobin levels at baseline and post-surgery in the two groups. The mean postoperative heart rate was significantly lower in the GSA compared to the GA (72.9±8.2 vs 81.5±11.5, P=0.007). No statistically significant differences in heart rate were found in the within-group comparisons. No statistically significant difference in mean pre- and postoperative O2Sat was observed between the two anesthesia techniques or within each technique. In both methods, postoperative pain was significantly reduced compared to preoperative levels (P<0.001). The mean postoperative pain in the GSA was significantly lower than in the GA (2.6±1.9 vs 3.9±1.8, P=0.005). No statistically significant difference in hemoglobin levels was observed before and after surgery between the two groups. However, for both methods, hemoglobin levels decreased significantly after surgery compared to before (P<0.001).
Additionally, the repeated-measures ANOVA revealed significant main effects of groups and time on systolic (Ptime<0.001; Pgroup=0.005), diastolic (Ptime<0.001; Pgroup=0.049), and MAP (Ptime<0.001; Pgroup=0.011). However, no significant interaction between the group and time was observed (Table 4 and Figure 2). As shown in Table 4, the GSA group consistently exhibited lower blood pressure compared to the GA group at all-time points. This finding indicates that GSA was consistently superior to GA in terms of blood pressure throughout the observation period.
4. Discussion
The desired anesthetic technique should have a prompt onset and reversal of effects. It should also maintain stable hemodynamics throughout the procedure without increasing the need for blood transfusion. Finally, an ideal anesthetic should shorten recovery room time while serving as an agent against postoperative pain, nausea, and vomiting, or as a supplement to analgesics [16]. Combining two anesthetic techniques, considering the proposed benefits and drawbacks of the other, is not new [26]. Therefore, this randomized clinical trial compared perioperative and postoperative parameters in 45 patients undergoing GA versus combined spinal and GA during LSF surgery. These results have significant implications for the differences in the effects of both anesthetic techniques on operative time, cardiovascular stability, postoperative analgesia, and hemodynamic parameters.
A standout finding was the significant decrease in operative time in the combined spinal and GA group compared with the GA alone group (128.6±47.0 vs 160.9±57.3 minutes, P=0.048). This implies that the additional use of SA facilitates more efficient surgical procedures. This decrease is associated with improved hemodynamic stability, less intraoperative blood loss, and a better surgical field for the surgeon, enabling a more efficient surgical process. One study found no statistically significant difference between the SA and GA groups about operative time [27]; however, the literature on combined spinal and GA indicates an association between its use and a decrease in surgery duration compared with GA alone, particularly in lumbar spine surgeries. This decrease may be attributed to improved hemodynamic stability, decreased intraoperative blood loss, and improved surgical field conditions, which make for a more efficient surgical process [16]. Induced hypotension during spine surgery offers the added benefits of reduced blood loss and the requirement for blood transfusion [28], better operating conditions, and shorter surgical time. Combined spinal and GA can greatly reduce the actual operating time compared to GA alone. This is chiefly due to better hemodynamic stability, decreased intraoperative blood loss, and improved surgical conditions. Hence, the results favor the application of combined spinal and GA as a safe and effective anesthetic technique for specific surgical procedures. Additionally, considering the equalization of preoperative preparation time between the groups in our study, with both groups having a median preservation time of 30 minutes, the variation in operative time was seemingly independent of any potential pre-surgical delay and was accounted for by the anesthetic technique employed.
Heart rate, a significant indicator of the autonomic and hemodynamic responses to surgical stress, showed significant differences between groups postoperatively. Baseline heart rates were similar in both groups; however, the combined spinal-GA group had a lower median postoperative heart rate (73 beats per minute) compared to the GA group (83 beats per minute), and this difference was statistically significant (P=0.007). More importantly, no significant difference was observed between the groups immediately following intubation or during surgery, suggesting that the SA-based heart rate stability benefits were most evident only during the postoperative phase. Research has shown that patients who have undergone combined spinal and GA might have more stable and acceptable heart rate levels during surgery compared with patients who would receive GA alone. For example, a randomized trial for laparoscopic hysterectomy revealed better hemodynamic stability throughout the surgical procedure, including heart rate, in the combined spinal-GA group versus the GA group alone [26].
In a study focusing on patients undergoing coronary artery bypass surgery (CABG), those who received combined spinal-GA maintained a comparatively stable heart rate compared to those who received only GA. The mean heart rate was significantly improved in the combined group, suggesting better hemodynamic stability throughout the surgical procedure [29]. With SA, hypotension and bradycardia can occur due to sympathetic blockade, especially with higher block levels or in more susceptible individuals [30-32]. Hence, the combined technique may reduce the need for interventional drugs, such as beta-blockers or vasopressors to modulate heart rate changes compared to GA. The various hemodynamic benefits of combined spinal and GA are further emphasized by the alterations noted in the systolic, diastolic, and MAP during the operative phases. At maximal surgical interventions, such as incision (112 vs 127 mmHg, P<0.001) and 30 minutes post-incision (105 vs 118 mmHg, P<0.001), systolic pressure was significantly lower in the combined spinal and GA group.
Likewise, MAP was lower in the GSA group at the time of incision and thereafter at measured intervals (P=0.037, <0.001). One study showed that when SA is supplemented with GA, the sympathectomy induced by SA may counteract increases in systemic vascular resistance, thereby targeting the elevated MAP [26]. While concerns regarding hypotension generated by spinal anesthetics have been raised by some practitioners [33-35], no significant hypotension (defined as a decrease in MAP of more than 20%) was observed in our combined spinal and GA group (P=0.885), thus reinforcing that it is a safe technique when well managed.
Another area of benefit identified has been postoperative pain management, in which combined spinal and GA has shown superiority. The postoperative VAS scores of the combined spinal and GA group were significantly lower than those of the GA group (median 3.0 vs 4.0, P=0.005). Several authors have reported that combined spinal and GA provides better postoperative analgesia than GA alone. For instance, in abdominal hysterectomy, patients with combined spinal and GA had lower pain scores and required fewer postoperative analgesics than those with GA alone [36]. Similarly, in robotic sacrocervicopexy, patients anesthetized with a combination of spinal and GA reported significantly lower pain scores and less analgesic intake during the immediate postoperative period. Pain and analgesic use within the first 24 hours after robotic gynecologic surgery was significantly lower when GSA was used compared to GA alone.
A considerably higher number of GA patients requested additional analgesic medications when they reached the recovery unit, compared to a few patients who underwent combined anesthesia. The lower reported pain levels in the study group may be associated with the analgesia provided by intrathecal anesthesia [37]. This decrease in opioid consumption is crucial to prevent opioid-associated side effects and fast-tracking recovery. One study indicated that adding spinal or regional blocks to GA markedly reduces intraoperative and postoperative opioid requirements. During breast surgery, patients receiving regional block (Pecs II) plus GA consumed fewer opioids intra- and postoperatively and had lower pain scores for up to 24 hours after surgery [38]. The repeated-measures analysis of pain scores over time showed a significant group effect and a group-by-time interaction, indicating that the analgesic benefit of SA persisted and was consistent across time points.
The recovery time in the post-anesthesia care unit did not differ significantly between groups, with median times of 27.5 minutes and 30 minutes (P=0.474). This suggests that the benefits of GSA regarding operative time and pain management do not necessarily lead to a faster, immediate recovery.
The lower hemoglobin levels after surgery in both groups correlated well with the expected surgical blood loss (P<0.001). Thus it is unsurprising that perioperative bleeding was unrelated to the anesthesia method of choice, as the bleeding volumes and requirements for transfusion did not differ significantly between groups. It is reassuring in the face of concerns that regional anesthesia (RA) would increase bleeding due to vasodilation caused by sympathectomy [39]. In other words, we believe that when good surgical techniques are used, carefully selected patients can undergo combined GSA without hemostatic risk.
Despite these promising results, some disadvantages deserve attention. The small sample size (n=45) limits the generalizability of the findings, and the single-center design may have reduced variability in surgical techniques and patient demographics. While the baseline characteristics were statistically comparable between the groups, unmeasured confounders, such as intraoperative fluid management, anesthesiologists’ experience, and postoperative analgesic protocols, may influence outcomes. Larger multicenter randomized trials stratified by type of surgery and with longer follow-up periods should be conducted in the future to confirm and further build on these findings.
5. Conclusion
In conclusion, evidence from this clinical trial indicates that combined GSA provides more definitive benefits over GA alone in patients undergoing LSF surgery. Such benefits include shorter operative durations, improved postoperative heart rate regulation, more consistent intraoperative blood pressure, and better pain control in the immediate postoperative period. These advantages favor the use of SA adjuncts in appropriate surgical groups to maintain perioperative hemodynamic stability with comfort, without compromising recovery duration or increasing the risk of bleeding. These results are of great importance in guiding anesthesia practices to optimize patient outcomes and reduce perioperative risks.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Guilan University of Medical Sciences, Rasht, Iran (Code: IR.GUMS.REC.1403.146) and conducted by the Code of Ethics of the World Medical Association (Declaration of Helsinki). The study protocol was approved by the Iranian Registry of Clinical Trials (IRCT), Tehran, Iran (Code: IRCT20140310016917N11). Informed consent was obtained from all participants before their inclusion in the study.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conception and study design: Afshin Mardvar, Ali Ashraf, Zoheir Reihanian and Mahdie Torkashvand; Data collection: Afshin Mardvar, Ali Ashraf, Zoheir Reihanian, Seifollah Jafari and Morteza Modaenama; Data analysis and interpretation: Ali Ashraf and Mohammadali Yazdanipour; Drafting the article: Afshin Mardvar, Ali Ashraf and Mohammadali Yazdanipour; Critical revision of the article: Ali Ashraf, Zoheir Reihanian and Morteza Modaenama; Final Approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgements
The authors acknowledge the assistance of Poursina Clinical Research Development Unit.
References
- Lall M. Nursing care of the patient undergoing lumbar spinal fusion. Journal of Nursing Education and Practice. 2018; 8(5):44. [DOI:10.5430/jnep.v8n5p44]
- Toivonen LA, Häkkinen A, Pekkanen L, Kyrölä K, Kautiainen H, Neva MH. Benefits of lumbar spine fusion surgery reach 10 years with various surgical indications. North American Spine Society Journal. 2023; 16:100276. [DOI:10.1016/j.xnsj.2023.100276] [PMID]
- Fritzell P, Hägg O, Wessberg P, Nordwall A; Swedish Lumbar Spine Study Group. 2001 volvo award winner in clinical studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: A multicenter randomized controlled trial from the Swedish lumbar spine study group. Spine. 2001; 26(23):2521-32. [DOI:10.1097/00007632-200112010-00002] [PMID]
- Weinstein JN, Tosteson TD, Lurie JD, Tosteson AN, Blood E, Hanscom B, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. New England Journal of Medicine. 2008; 358(8):794-810. [DOI:10.1056/NEJMoa0707136] [PMID]
- Saifi C, Cazzulino A, Laratta J, Save AV, Shillingford JN, Louie PK, et al. Utilization and economic impact of posterolateral fusion and posterior/transforaminal lumbar interbody fusion surgeries in the United States. Global Spine Journal. 2019; 9(2):185-90. [DOI:10.1177/2192568218790557] [PMID]
- de Kunder SL, Rijkers K, Caelers I, de Bie RA, Koehler PJ, van Santbrink H. Lumbar interbody fusion: A historical overview and a future perspective. Spine. 2018; 43(16):1161-8. [DOI:10.1097/BRS.0000000000002534] [PMID]
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical research council guidance. BMJ. 2015; 350:h1258. [DOI:10.1136/bmj.h1258] [PMID]
- Damsgaard JB, Jørgensen LB, Norlyk A, Birkelund R. Spinal fusion surgery: From relief to insecurity. International Journal of Orthopaedic and Trauma Nursing. 2017; 24:31-9. [DOI:10.1016/j.ijotn.2016.06.001] [PMID]
- van der Horst AY, Trompetter HR, Pakvis DFM, Kelders SM, Schreurs KMG, Bohlmeijer ET. Between hope and fear: A qualitative study on perioperative experiences and coping of patients after lumbar fusion surgery. International Journal of Orthopaedic and Trauma Nursing. 2019; 35:100707. [DOI:10.1016/j.ijotn.2019.07.003] [PMID]
- Archer K, Bird ML, Haug C, Coronado R, Wegener S, Devin CJ, et al. Patients’ experience and expectations of lumbar spine surgery for degenerative conditions: A qualitative study. The Spine Journal. 2015; 15(10):S99-S100. [DOI:10.1016/j.spinee.2015.07.046]
- Hulscher ME, Laurant MG, Grol RP. Process evaluation on quality improvement interventions. Quality & Safety in Health Care. 2003; 12(1):40-6. [DOI:10.1136/qhc.12.1.40] [PMID]
- Amoroso K, Hughes AP, Soffin EM. Spine surgery under neuraxial vs. general anesthesia: The current state of comparative outcomes research. Current Opinion in Anaesthesiology. 2023; 36(5):516-24. [DOI:10.1097/ACO.0000000000001294] [PMID]
- Lessing NL, Edwards CC, Brown IV CH, Ledford EC, Dean CL, Lin C, et al. Spinal anesthesia in elderly patients undergoing lumbar spine surgery. Orthopedics. 2017; 40(2):e317-e22. [DOI:10.3928/01477447-20161219-01]
- Lessing NL, Edwards CC, Dean CL, Waxter OH, Lin C, Curto RA, et al. Spinal anesthesia for geriatric lumbar spine surgery: A comparative case series. International Journal of Spine Surgery. 2020; 14(5):713-21. [DOI:10.14444/7103] [PMID]
- Meng T, Zhong Z, Meng L. Impact of spinal anaesthesia vs. general anaesthesia on peri-operative outcome in lumbar spine surgery: A systematic review and meta-analysis of randomised, controlled trials. Anaesthesia. 2017; 72(3):391-401. [DOI:10.1111/anae.13702] [PMID]
- Attari MA, Mirhosseini SA, Honarmand A, Safavi MR. Spinal anesthesia versus general anesthesia for elective lumbar spine surgery: A randomized clinical trial. Journal of Research in Medical Sciences. 2011; 16(4):524. [PMID]
- Jellish WS, Thalji Z, Stevenson K, Shea J. A prospective randomized study comparing short-and intermediate-term perioperative outcome variables after spinal or general anesthesia for lumbar disk and laminectomy surgery. Anesthesia & Analgesia. 1996; 83(3):559-64. [DOI:10.1097/00000539-199609000-00021]
- McLain RF, Kalfas I, Bell GR, Tetzlaff JE, Yoon HJ, Rana M. Comparison of spinal and general anesthesia in lumbar laminectomy surgery: A case-controlled analysis of 400 patients. Journal of Neurosurgery: Spine. 2005; 2(1):17-22. [DOI:10.3171/spi.2005.2.1.0017] [PMID]
- Tetzlaff JE, Dilger JA, Kodsy M, Al-Bataineh J, Yoon HJ, Bell GR. Spinal anesthesia for elective lumbar spine surgery. Journal of Clinical Anesthesia. 1998; 10(8):666-9. [DOI:10.1016/S0952-8180(98)00112-3] [PMID]
- Chen HT, Tsai CH, Chao SC, Kao TH, Chen YJ, Hsu HC, et al. Endoscopic discectomy of L5-S1 disc herniation via an interlaminar approach: Prospective controlled study under local and general anesthesia. Surgical Neurology International. 2011; 2:93. [DOI:10.4103/2152-7806.82570] [PMID]
- McLain RF, Tetzlaff JE, Bell GR, Uwe-Lewandrowski K, Yoon HJ, Rana M. Microdiscectomy: Spinal anesthesia offers optimal results in general patient population. Journal of Surgical Orthopaedic Advances. 2007; 16(1):5-11. [PMID]
- Subbiah M, Madhuvarshinee KM, Vinothan RJS, Poornima V, Ramanarayanan R, Manikandan B, et al. A novel combined anesthetic technique to improve the surgical working conditions of lumbar and thoracolumbar spine surgery from a spine surgeon’s perspective: A prospective randomized controlled study. Asian Spine Journal. 2023; 17(2):285-92. [DOI:10.31616/asj.2022.0198] [PMID]
- Parker MJ, Unwin SC, Handoll HH, Griffiths R. General versus spinal/epidural anaesthesia for surgery for hip fractures in adults. The Cochrane Database of Systematic Reviews. 2000; (4):CD000521. [DOI:10.1002/14651858.CD000521] [PMID]
- Kahl C, Cleland JA. Visual analogue scale, numeric pain rating scale and the McGill pain questionnaire: An overview of psychometric properties. Physical Therapy Reviews. 2005; 10(2):123-8. [DOI:10.1179/108331905X55776]
- Sadrolsadat SH, Mahdavi AR, Moharari RS, Khajavi MR, Khashayar P, Najafi A, et al. A prospective randomized trial comparing the technique of spinal and general anesthesia for lumbar disk surgery: A study of 100 cases. Surgical Neurology. 2009; 71(1):60-5. [DOI:10.1016/j.surneu.2008.08.003] [PMID]
- Ghodki PS, Sardesai SP, Naphade RW. Combined spinal and general anesthesia is better than general anesthesia alone for laparoscopic hysterectomy. Saudi Journal of Anaesthesia. 2014; 8(4):498-503. [DOI:10.4103/1658-354X.140864] [PMID]
- Yucel MO, Çift A, Benlioglu C, Kalyenci B, Sever S, Çoban F, et al. Comparison of the efficacy of spinal and general anesthesia in retrograde intrarenal surgery. Medical Journal of Islamic World Academy of Sciences. 2023; 30(1):1-6. [DOI:10.5505/ias.2023.40316]
- Eva Y, Cheung WY, Ng KF, Luk KD. Reducing perioperative blood loss and allogeneic blood transfusion in patients undergoing major spine surgery. The Journal of Bone and Joint Surgery. 2011; 93(13):1268-77. [DOI:10.2106/JBJS.J.01293] [PMID]
- Firoozabadi MD, Ebadi A, Sheikhi MA, Rahmani H. Effect of general anesthesia plus spinal anesthesia on patients hemodynamic during coronary artery bypass Grafting surgery. Der Pharma Chemica. 2016; 8:301-5. [Link]
- Carpenter RL, Caplan RA, Brown DL, Stephenson C, Wu R. Incidence and risk factors for side effects of spinal anesthesia. Anesthesiology. 1992; 76(6):906-16. [DOI:10.1097/00000542-199206000-00006] [PMID]
- Gebrargs L, Gebremeskel B, Aberra B, Hika A, Yimer Y, Weldeyohannes M, et al. Comparison of hemodynamic response following spinal anesthesia between controlled hypertensive and normotensive patients undergoing surgery below the umbilicus: An observational prospective cohort study. Anesthesiology Research and Practice. 2021; 2021(1):8891252. [DOI:10.1155/2021/8891252] [PMID]
- Movasseghi G, Hassani V, Mohaghegh MR, Safaeian R, Safari S, Zamani MM, et al. Comparison between spinal and general anesthesia in percutaneous nephrolithotomy. Anesthesiology and Pain Medicine. 2013; 4(1):e13871. [DOI:10.5812/aapm.13871] [PMID]
- Andemeskel Y, Brhane D, MohammedAli J, Habtetsion T. Comparison of crystalloid preloading versus ephedrine prophylaxis to prevent spinal anesthesia induced hypotension during cesarean delivery: A randomized clinical trial. Anesthesia and Critical Care. 2024; 6(2024):17-25. [DOI:10.26502/acc.067]
- Ferré F, Martin C, Bosch L, Kurrek M, Lairez O, Minville V. Control of spinal anesthesia-induced hypotension in adults. Local and Regional Anesthesia. 2020; 13:39-46. [DOI:10.2147/LRA.S240753] [PMID]
- Hofhuizen C, Lemson J, Snoeck M, Scheffer GJ. Spinal anesthesia-induced hypotension is caused by a decrease in stroke volume in elderly patients. Local and Regional Anesthesia. 2019; 12:19-26. [DOI:10.2147/LRA.S193925] [PMID]
- Catarci S, Zanfini BA, Capone E, Vassalli F, Frassanito L, Biancone M, et al. Blended (combined spinal and general) vs. general anesthesia for abdominal hysterectomy: A retrospective study. Journal of Clinical Medicine. 2023; 12(14):4775. [DOI:10.3390/jcm12144775] [PMID]
- Segal D, Awad N, Nasir H, Mustafa S, Lowenstein L. Combined spinal and general anesthesia vs general anesthesia for robotic sacrocervicopexy: A randomized controlled trial. International Urogynecology Journal. 2014; 25(3):369-74. [DOI:10.1007/s00192-013-2194-8] [PMID]
- Senapathi TGA, Widnyana IMG, Aribawa IGNM, Jaya AGPS, Junaedi IMD. Combined ultrasound-guided Pecs II block and general anesthesia are effective for reducing pain from modified radical mastectomy. Journal of Pain Research. 2019; 12:1353-8. [DOI:10.2147/JPR.S197669] [PMID]
- Malinzak EB, Gan TJ. Regional anesthesia for vascular access surgery. Anesthesia and Analgesia. 2009; 109(3):976-80. [DOI:10.1213/ane.0b013e3181adc208] [PMID]a
| Rights and Permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
