Thu, Jul 3, 2025
Volume 2, Issue 3 (12-2016)
Iran J Neurosurg 2016, 2(3): 26-28 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sharifi G, Alimohammadi E, Ebrahimzadeh K, Moradian K, Rezaei O. Huge Sequestered Spinal Disc Mimicking Spinal Intradural Tumor. Iran J Neurosurg 2016; 2 (3) :26-28
URL: http://irjns.org/article-1-62-en.html
URL: http://irjns.org/article-1-62-en.html



1- Associate Professor, Shahid Beheshti University of Medical Sciences, Loghman Hakim Hospital, Tehran, Iran
2- Resident of Neurosurgery, Shahid Beheshti University of Medical Sciences, Loghman Hakim Hospital, Tehran, Iran
3- Assistant Professor of Neurosurgery, Shahid Beheshti University of Medical Sciences, Loghman Hakim Hospital, Tehran, Iran
4- Professor of Neurosurgery, Shahid Beheshti University of Medical Sciences, Loghman Hakim Hospital, Tehran, Iran
2- Resident of Neurosurgery, Shahid Beheshti University of Medical Sciences, Loghman Hakim Hospital, Tehran, Iran
3- Assistant Professor of Neurosurgery, Shahid Beheshti University of Medical Sciences, Loghman Hakim Hospital, Tehran, Iran
4- Professor of Neurosurgery, Shahid Beheshti University of Medical Sciences, Loghman Hakim Hospital, Tehran, Iran
Full Text [PDF 1245 kb]
(4880 Downloads)
| Abstract (HTML) (6667 Views)
.jpg)

Full Text: (2311 Views)
Background and Importance
Disk sequestration can be defined as a herniated disk with perforation of the fibrous ring (or outermost annulus fibrosus) and posterior longitudinal ligament with migration of the disk fragment to the epidural space. Even after the introduction of high-resolution magnetic resonance imaging (MRI), it is still misinterpreted as neoplastic masses [1-3]. Unfortunately, no particular symptoms or signs are also known to allow differentiation between atypical hernias and spinal tumors. Rarely, a giant sequestered fragment without creating any significant changes and not affiliated with the disk distance can be seen on the channel. Therefore, it is mixed with spinal tumors [2,4]. MRI findings are useful in the preoperative diagnosis of disc herniation. The differential diagnosis includes not only isointensely metastatic lesions but also some other benign epidural lesions such as synovial cysts, hematomas, and abscesses [5,6]. A case of a huge herniated and sequestrated disc, which is misinterpreted as a spinal tumor on the radiological report is presented here.
Case Presentation
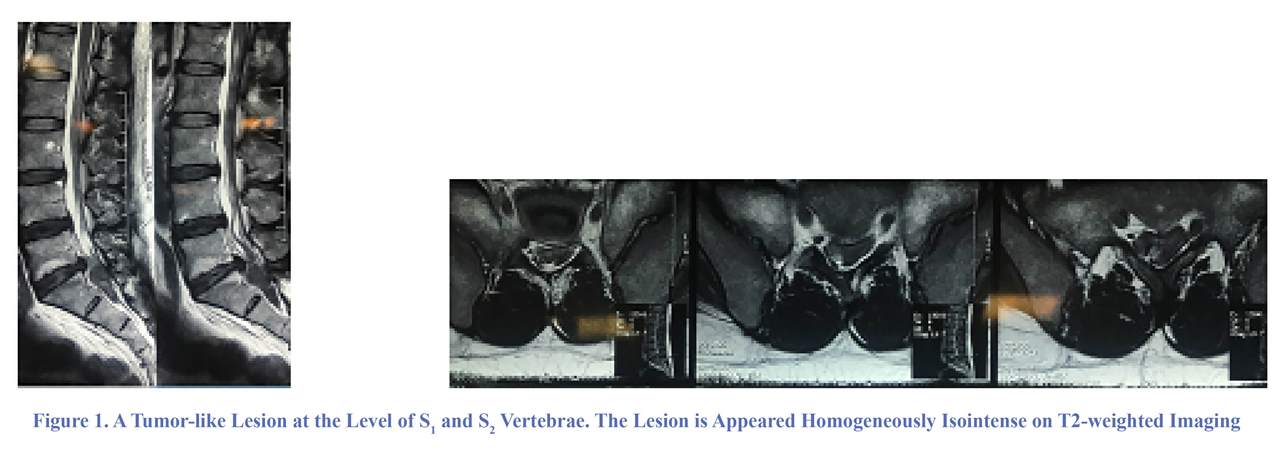
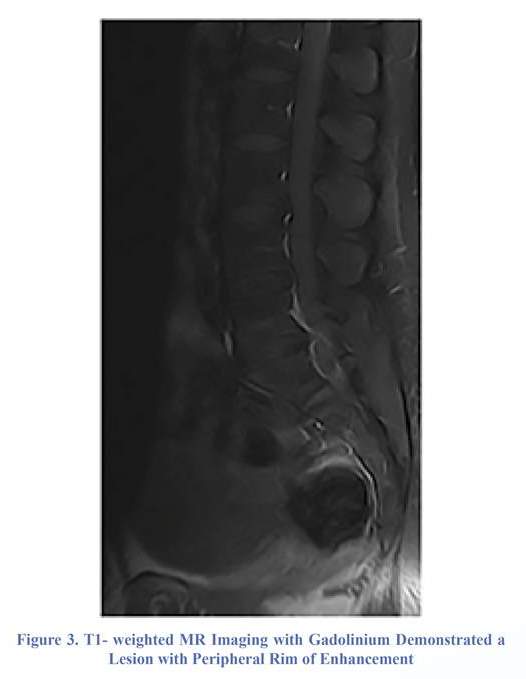
A 36-year-old man was admitted to our hospital with complaint of low back pain and left lower extremity pain and weakness since about two months ago, whose condition exacerbated suddenly four days before admission. His neurological status showed no detectable muscle atrophy. Neurological examination revealed positive Lasègue's sign and sensory deficit over the L5 and S1 dermatomes in both sides especially left side. Deep tendon reflexes were inattentive at the knee and ankle, and the motor power in terms of ankle dorsiflexion and great toe dorsiflexion was 3/5 in left lower limb. Bladder and bowel functions were intact at all. By radiological evaluation, MRI revealed a tumor-like lesion at the level of S1 and S2 vertebrae. The lesion is appeared homogeneously isointense on T2-weighted imaging (Figure 1) and slightly hypointense on T1-weighted imaging (Figure 2). T1-weighted MR imaging with gadolinium demonstrated a lesion with peripheral rim of enhancement (Figure 3).
The patient underwent L5-S1 and S1-S2 laminectomy, in preparation for an oncological operation. However, investigation of the epidural space unexpectedly found a huge mass, which was easily removed totally from the left vertebral canal with the macroscopic appearance of a sequestrated disc (Figure 4). The fragment was probably delivered from the L5-S1 level, but it was completely detached from the disc space. By a meticulous investigation under microscope, a tear of the annulus was identified at the L5-S1 level. The patient's postoperative course was ordinary and he demonstrated full pain free recovery within a month and the force of his left lower limb was become 5/5 after a weak. Histopathological examination confirmed the presence of disc material without neoplastic activity.
Discussion
Only isolated case reports describing sequestrated disc fragments simulating intraspinal benign or malignant space-occupying lesions have been published [1,3,6]. Unusual presentation of sequestrated disc fragments on preoperative
Disk sequestration can be defined as a herniated disk with perforation of the fibrous ring (or outermost annulus fibrosus) and posterior longitudinal ligament with migration of the disk fragment to the epidural space. Even after the introduction of high-resolution magnetic resonance imaging (MRI), it is still misinterpreted as neoplastic masses [1-3]. Unfortunately, no particular symptoms or signs are also known to allow differentiation between atypical hernias and spinal tumors. Rarely, a giant sequestered fragment without creating any significant changes and not affiliated with the disk distance can be seen on the channel. Therefore, it is mixed with spinal tumors [2,4]. MRI findings are useful in the preoperative diagnosis of disc herniation. The differential diagnosis includes not only isointensely metastatic lesions but also some other benign epidural lesions such as synovial cysts, hematomas, and abscesses [5,6]. A case of a huge herniated and sequestrated disc, which is misinterpreted as a spinal tumor on the radiological report is presented here.
Case Presentation
A 36-year-old man was admitted to our hospital with complaint of low back pain and left lower extremity pain and weakness since about two months ago, whose condition exacerbated suddenly four days before admission. His neurological status showed no detectable muscle atrophy. Neurological examination revealed positive Lasègue's sign and sensory deficit over the L5 and S1 dermatomes in both sides especially left side. Deep tendon reflexes were inattentive at the knee and ankle, and the motor power in terms of ankle dorsiflexion and great toe dorsiflexion was 3/5 in left lower limb. Bladder and bowel functions were intact at all. By radiological evaluation, MRI revealed a tumor-like lesion at the level of S1 and S2 vertebrae. The lesion is appeared homogeneously isointense on T2-weighted imaging (Figure 1) and slightly hypointense on T1-weighted imaging (Figure 2). T1-weighted MR imaging with gadolinium demonstrated a lesion with peripheral rim of enhancement (Figure 3).
The patient underwent L5-S1 and S1-S2 laminectomy, in preparation for an oncological operation. However, investigation of the epidural space unexpectedly found a huge mass, which was easily removed totally from the left vertebral canal with the macroscopic appearance of a sequestrated disc (Figure 4). The fragment was probably delivered from the L5-S1 level, but it was completely detached from the disc space. By a meticulous investigation under microscope, a tear of the annulus was identified at the L5-S1 level. The patient's postoperative course was ordinary and he demonstrated full pain free recovery within a month and the force of his left lower limb was become 5/5 after a weak. Histopathological examination confirmed the presence of disc material without neoplastic activity.
Discussion
Only isolated case reports describing sequestrated disc fragments simulating intraspinal benign or malignant space-occupying lesions have been published [1,3,6]. Unusual presentation of sequestrated disc fragments on preoperative
MRI is extremely rare. A recent report by Carvi y Nievas MN et al. found that only 11 of 3000 patients suffering from lumbar disc herniation were mistaken for another spinal space-occupying lesion [2]. It is usually not difficult with current MRI techniques to differentiate lumbar disc herniation from other conditions [7]. However, rare sequestrated disc fragments may still be mistaken for other neoplastic or non-neoplastic lesions. Complete detachment and migration, even intra- or extradurally, as well as extraordinarily large dimensions of the disc fragment are two of the commonest reasons of this confusion. Atypical sequestrated disc herniations usually appear as heterogeneously hypointense to isointense on T1- weighted sequences and hypointense or hyperintense on T2-weighted MR images, depending on location (intra- or extradural) and time of evolution [1,2,8]. MRI with contrast medium is useful to differentiate herniated disc from tumors and other epidural lesions, as the non-enhancing disc fragment is commonly associated with peripheral enhancement. Herniated disc fragment rarely includes central enhancement, a finding attributed to vascular granulation tissue infiltrating the fragment, but is never associated with enhancement of the spinal meninges, an early characteristic finding of neoplastic lesions such as lymphoma, neurofibroma, neuroblastoma, mesothelioma, and lung cancer [2,9,10]. Contrast-enhanced MRI scans are useful to differentiate a herniated disc from a disc space infection or tumor. Likewise in our case, peripheral enhancement around the nonenhancing disc fragment is commonly seen on contrast MRI. A herniated disc fragment will rarely enhance centrally, which is attributed to vascular granulation tissue infiltrating the fragment [2,11]. In our case, the lesion appeared homogeneously isointense on T2-weighted MR imaging (Figure 1), that let us suspect a neoplastic lesion, but MRI with contrast medium showed peripheral enhancement of the rim of the lesion (Figure 3), which is typical appearance of a disc fragment. Nevertheless, the large size and shape of the lesion were confusing, leading us to misinterpret its nature, since lumbar disc herniations are usually much smaller and round. A further factor of confusion was the fact that no clear radiological evidence was found of any possible connection of the mass to adjacent disc space without either reduction of disc space height or changes of obvious disc color on MRI (Figures 1 & 2), misleading us from suspecting a sequestrated disc fragment. Corresponding to imaging which showed peripheral engulfment of lesion by CSF, the lesion was considered to be located in the intradural compartment.
Conclusion
Although uncommon, sequestered disc herniation can mimic tumors and other spinal occupying-space lesions, being difficult to distinguish in view of the variety of imaging presentation. Sequestrated lumbar disc fragments should always be considered in the differential diagnosis of mass lesions of the spinal canal, and even when their shape and voluminous size are unusual.
Funding
None.
Conflicts of Interest
The authors declare no conflict of interest.
Author’s Contribution
Conception and Design: Guive Sharifi. Data Collection: Karim Moradian. Drafting the Article: Kaveh Ebrahimzadeh. Critical Revising the Article: Ehsan Alimohammadi. Reviewing Submitted Version of Manuscript: Omidvar Rezaei. Approving the Final Version of the Manuscript: Ehsan Alimohammadi.
References
1. Schellinger D, Manz H, Vidic B, Patronas N, Deveikis J, Muraki A, et al. Disk fragment migration. Radiology. 1990;175(3):831-6.
2. Nievas MNC, Hoellerhage H-G. Unusual sequestered disc fragments simulating spinal tumors and other space-occupying lesions: clinical article. Journal of Neurosurgery: Spine. 2009;11(1):42-8.
3. Aydin M, Ozel S, Sen O, Erdogan B, Yildirim T. Intradural disc mimicking: a spinal tumor lesion. Spinal Cord. 2004;42(1):52-4.
4. Göçmez C, Kamaşak K, Başarslan SK, Ceviz A. Huge sequestered spinal disc with tumor appearance: a case report. Mustafa Kemal Üniversitesi Tıp Dergisi. 2013;4(15).
5. Lidov M, Stollman A, Casden A, Som P, Bederson J. MRI of lumbar intradural disc herniation. Clinical imaging. 1994;18(3):173-8.
6. Őzer E, Yurtsever C, Yücesoy K, Güner M. Lumbar intraradicular disc
herniation: report of a rare and preoperatively unpredictable case and review of the literature. The Spine Journal. 2007;7(1):106-10.
7. Ramsey RG, Geremia GK. CNS complications of AIDS: CT and MR findings. American Journal of Roentgenology. 1988;151(3):449-54.
8. Saruhashi Y, Omura K, Miyamoto K, Katsuura A, Hukuda S. A migrated lumbar disc herniation simulating a dumbbell tumor. Journal of Spinal Disorders & Techniques. 1999;12(4):307-9.
9. Glickstein MF, Burke Jr DL, Kressel HY. Magnetic resonance demonstration of hyperintense herniated discs and extruded disc fragments. Skeletal radiology. 1989;18(7):527-30.
10. Hwang GJ, Suh JS, Na JB, Lee HM, Kim NH. Contrast enhancement pattern and frequency of previously unoperated lumbar discs on MRI. Journal of Magnetic Resonance Imaging. 1997;7(3):575-8.
11. Masaryk TJ, Ross JS, Modic MT, Boumphrey F, Bohlman H, Wilber G. High-resolution MR imaging of sequestered lumbar intervertebral disks. American journal of neuroradiology. 1988;9(2):351-8.
Comments
Respected authors have reported a case with Huge Sequestered Spinal Disc resembling lumbar spinal canal tumor, it was hyperintense on T2W, rim enhancing after gadolinium injection on T1W and totally separated from disc space.
Non typical sequestrated disc herniation is extremely rare (0.4%) and can usually be identified only during surgery. Further exploration in such cases frequently reveals that disc space is completely empty, which indicates that the sequestered disc fragment has come from offending disc space. Such lesions are sometimes encased by cystoid adipose tissue which show high-intensity signal on the T1-weighted and T2-weighted images. Peripheral enhancement around the nonenhancing disc fragment (explained by inflammatory reaction and neovascularization around the sequestered disc fragment) is typical for a disc fragment. Malignancies typically show homogeneous or heterogeneous uptake, and rarely ring enhancement. Chondrosarcomas may show moderate peripheral enhancement, but have lobulate architecture, differing from the disc fragment. Metastases commonly affect the adjacent bones and have a wide variety of signals. Nerve sheath tumors are isointense on T1W and hyperintense on T2W, with enhancement after contrast infusion, resembling the sequestered fragment, however, are primarily intra-dural,situation that occurs very rarely in disc herniations. extra-dural hematomas may also provide contrast enhancement, but have trauma history associated. Still, there are situations where the disc fragment may show homogeneous enhancement, due to granulation tissue infiltration thus the diagnosis can become a challenge, hence, the suspicion of disc herniation should always be kept in mind while investigate an epidural mass.
Conclusion
Although uncommon, sequestered disc herniation can mimic tumors and other spinal occupying-space lesions, being difficult to distinguish in view of the variety of imaging presentation. Sequestrated lumbar disc fragments should always be considered in the differential diagnosis of mass lesions of the spinal canal, and even when their shape and voluminous size are unusual.
Funding
None.
Conflicts of Interest
The authors declare no conflict of interest.
Author’s Contribution
Conception and Design: Guive Sharifi. Data Collection: Karim Moradian. Drafting the Article: Kaveh Ebrahimzadeh. Critical Revising the Article: Ehsan Alimohammadi. Reviewing Submitted Version of Manuscript: Omidvar Rezaei. Approving the Final Version of the Manuscript: Ehsan Alimohammadi.
References
1. Schellinger D, Manz H, Vidic B, Patronas N, Deveikis J, Muraki A, et al. Disk fragment migration. Radiology. 1990;175(3):831-6.
2. Nievas MNC, Hoellerhage H-G. Unusual sequestered disc fragments simulating spinal tumors and other space-occupying lesions: clinical article. Journal of Neurosurgery: Spine. 2009;11(1):42-8.
3. Aydin M, Ozel S, Sen O, Erdogan B, Yildirim T. Intradural disc mimicking: a spinal tumor lesion. Spinal Cord. 2004;42(1):52-4.
4. Göçmez C, Kamaşak K, Başarslan SK, Ceviz A. Huge sequestered spinal disc with tumor appearance: a case report. Mustafa Kemal Üniversitesi Tıp Dergisi. 2013;4(15).
5. Lidov M, Stollman A, Casden A, Som P, Bederson J. MRI of lumbar intradural disc herniation. Clinical imaging. 1994;18(3):173-8.
6. Őzer E, Yurtsever C, Yücesoy K, Güner M. Lumbar intraradicular disc
herniation: report of a rare and preoperatively unpredictable case and review of the literature. The Spine Journal. 2007;7(1):106-10.
7. Ramsey RG, Geremia GK. CNS complications of AIDS: CT and MR findings. American Journal of Roentgenology. 1988;151(3):449-54.
8. Saruhashi Y, Omura K, Miyamoto K, Katsuura A, Hukuda S. A migrated lumbar disc herniation simulating a dumbbell tumor. Journal of Spinal Disorders & Techniques. 1999;12(4):307-9.
9. Glickstein MF, Burke Jr DL, Kressel HY. Magnetic resonance demonstration of hyperintense herniated discs and extruded disc fragments. Skeletal radiology. 1989;18(7):527-30.
10. Hwang GJ, Suh JS, Na JB, Lee HM, Kim NH. Contrast enhancement pattern and frequency of previously unoperated lumbar discs on MRI. Journal of Magnetic Resonance Imaging. 1997;7(3):575-8.
11. Masaryk TJ, Ross JS, Modic MT, Boumphrey F, Bohlman H, Wilber G. High-resolution MR imaging of sequestered lumbar intervertebral disks. American journal of neuroradiology. 1988;9(2):351-8.
Comments
Respected authors have reported a case with Huge Sequestered Spinal Disc resembling lumbar spinal canal tumor, it was hyperintense on T2W, rim enhancing after gadolinium injection on T1W and totally separated from disc space.
Non typical sequestrated disc herniation is extremely rare (0.4%) and can usually be identified only during surgery. Further exploration in such cases frequently reveals that disc space is completely empty, which indicates that the sequestered disc fragment has come from offending disc space. Such lesions are sometimes encased by cystoid adipose tissue which show high-intensity signal on the T1-weighted and T2-weighted images. Peripheral enhancement around the nonenhancing disc fragment (explained by inflammatory reaction and neovascularization around the sequestered disc fragment) is typical for a disc fragment. Malignancies typically show homogeneous or heterogeneous uptake, and rarely ring enhancement. Chondrosarcomas may show moderate peripheral enhancement, but have lobulate architecture, differing from the disc fragment. Metastases commonly affect the adjacent bones and have a wide variety of signals. Nerve sheath tumors are isointense on T1W and hyperintense on T2W, with enhancement after contrast infusion, resembling the sequestered fragment, however, are primarily intra-dural,situation that occurs very rarely in disc herniations. extra-dural hematomas may also provide contrast enhancement, but have trauma history associated. Still, there are situations where the disc fragment may show homogeneous enhancement, due to granulation tissue infiltration thus the diagnosis can become a challenge, hence, the suspicion of disc herniation should always be kept in mind while investigate an epidural mass.
Type of Study: Case report |
Subject:
Gamma Knife Radiosurgery
References
1. Schellinger D, Manz H, Vidic B, Patronas N, Deveikis J, Muraki A, et al. Disk fragment migration. Radiology. 1990;175(3):831-6. [DOI:10.1148/radiology.175.3.2343133] [PMID]
2. Nievas MNC, Hoellerhage H-G. Unusual sequestered disc fragments simulating spinal tumors and other space-occupying lesions: clinical article. Journal of Neurosurgery: Spine. 2009;11(1):42-8. [DOI:10.3171/2009.3.SPINE08161] [PMID]
3. Aydin M, Ozel S, Sen O, Erdogan B, Yildirim T. Intradural disc mimicking: a spinal tumor lesion. Spinal Cord. 2004;42(1):52-4. [DOI:10.1038/sj.sc.3101476] [PMID]
4. Göçmez C, Kamaşak K, Başarslan SK, Ceviz A. Huge sequestered spinal disc with tumor appearance: a case report. Mustafa Kemal Üniversitesi Tıp Dergisi. 2013;4(15).
5. Lidov M, Stollman A, Casden A, Som P, Bederson J. MRI of lumbar intradural disc herniation. Clinical imaging. 1994;18(3):173-8. [DOI:10.1016/0899-7071(94)90077-9]
6. Őzer E, Yurtsever C, Yücesoy K, Güner M. Lumbar intraradicular disc herniation: report of a rare and preoperatively unpredictable case and review of the literature. The Spine Journal. 2007;7(1):106-10. [DOI:10.1016/j.spinee.2006.04.011] [PMID]
7. Ramsey RG, Geremia GK. CNS complications of AIDS: CT and MR findings. American Journal of Roentgenology. 1988;151(3):449-54. [DOI:10.2214/ajr.151.3.449] [PMID]
8. Saruhashi Y, Omura K, Miyamoto K, Katsuura A, Hukuda S. A migrated lumbar disc herniation simulating a dumbbell tumor. Journal of Spinal Disorders & Techniques. 1999;12(4):307-9.
9. Glickstein MF, Burke Jr DL, Kressel HY. Magnetic resonance demonstration of hyperintense herniated discs and extruded disc fragments. Skeletal radiology. 1989;18(7):527-30. [DOI:10.1007/BF00351754] [PMID]
10. Hwang GJ, Suh JS, Na JB, Lee HM, Kim NH. Contrast enhancement pattern and frequency of previously unoperated lumbar discs on MRI. Journal of Magnetic Resonance Imaging. 1997;7(3):575-8. [DOI:10.1002/jmri.1880070319] [PMID]
11. Masaryk TJ, Ross JS, Modic MT, Boumphrey F, Bohlman H, Wilber G. High-resolution MR imaging of sequestered lumbar intervertebral disks. American journal of neuroradiology. 1988;9(2):351-8.
| Rights and Permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
