Sun, Jul 5, 2026
Volume 1, Issue 4 (3-2016)
Iran J Neurosurg 2016, 1(4): 11-14 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Haddadi K, Yosefzadeh F. Epidemiology of Traumatic Spinal Injury in north of Iran: A prospective Study. Iran J Neurosurg 2016; 1 (4) :11-14
URL: http://irjns.org/article-1-25-en.html
URL: http://irjns.org/article-1-25-en.html


1- MD, Assistant Professor, Department of Neurosurgery, Imam Khomeini Hospital, Orthopedic Research Center, Mazandaran University of Medical Sciences, Sari, Mazandaran, Iran
2- MD, School of Medicine, Mazandaran University of Medical Sciences, Sari, Mazandaran, Iran
2- MD, School of Medicine, Mazandaran University of Medical Sciences, Sari, Mazandaran, Iran
Full Text [PDF 509 kb]
(3073 Downloads)
| Abstract (HTML) (8469 Views)
Full Text: (3292 Views)
Introduction
Spinal cord injury (SCI) is a highly destructive situation (1) which is related to severe disability and death after trauma (2). Incidence of SCI is 12.1-57.8 cases per million (1) .The cost to the patient, their family and the health care system can be enormous (3).
In the US, spinal cord injury is the most costly traumatic condition. In a prospective population-based cohort study, Johnson et al. (4) reported that the costs for home care, services, and secondary medical complications reached almost $200,000 for each patient during the first two years after injury. The average cost of the first admission is approximately $95,203, with home modifications costing $8,203, medical services and equipment costing $7,866, and nurse and home care support costing $6,269 per year (5). An understanding of the epidemiology of SCI is essential for planning cost-effective care and for developing preventive strategies (6). Significant changes in SCI prevalence were observed among geographic locations, so these data are principal for local and regional health care economics (5). Rahimi-Movaghar et al. (2009) performed a population-based study to determine the prevalence of spine injury (SI) and spinal cord injury (SCI) in Tehran, Iran (7). The prevalence of traumatic SCI in Tehran ranged from 1.2 to 11.4 per 10,000 people.
Traumatic spine fracture (TSF) can occur as an isolated lesion or associated with other injuries such as to the spinal cord, head, extremities, and other organs injuries. Role of spine injury as a potential cause of disability and/or death is usually neglected. It commonly causes short-term disability (8), but may also result in long-term or even permament disability (9). Although the incidence of TSF increases in old population (5-8), it mostly involves young persons (10), which may increase the burden of this disease.
Although more than 80% of the world's population live in developing countries, little information is available regarding the epidemiology of SCI in these countries. The aim of the study was to determine regional epidemiology, demographics, mechanisms and severity of spine and spinal cord injury in a great area of north of Iran, Mazandaran.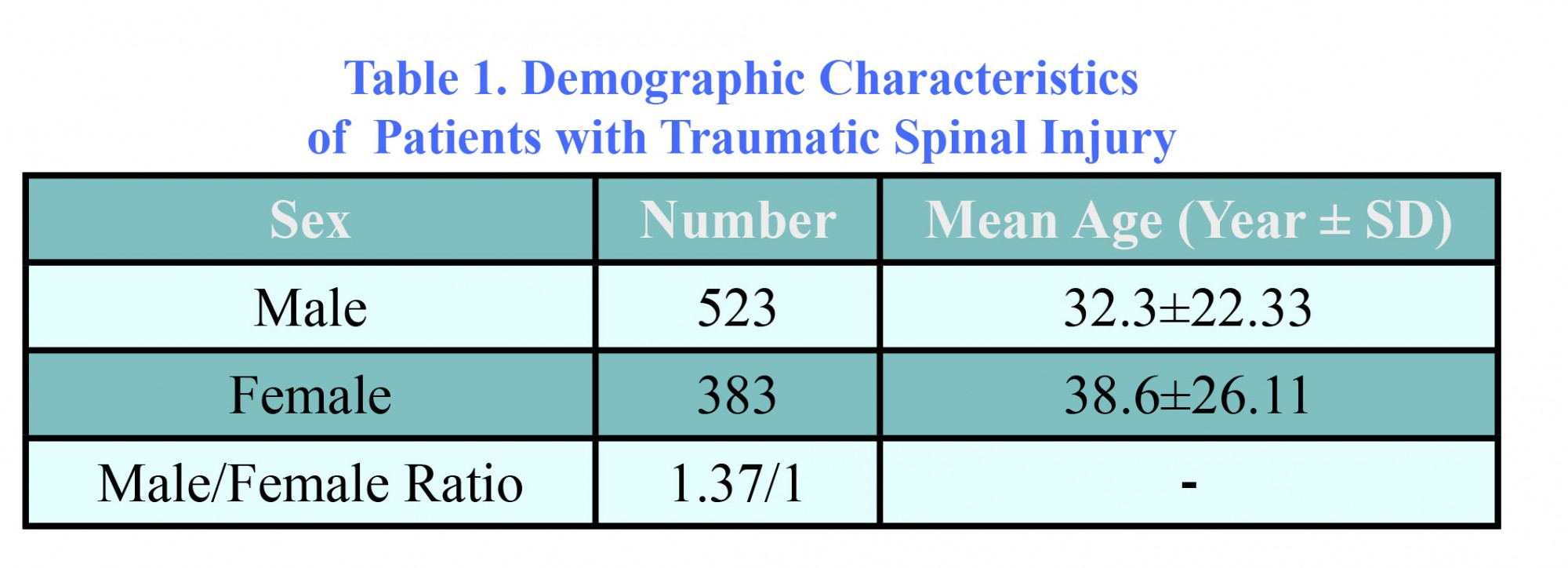

Variation of lifestyle in different countries and different regions of a country influence mechanism of trauma.
Yousefzadeh et al. (2008) showed thoracolumbar spine was common area for fracture (42). In our study, thoracolumbar spine was common involved area in traffic accidents, and thoracic spine was frequent site for falling. But Heidari et al. (2010) reported that cervical spine fractures were significantly common in road traffic accidents, and lumbar fractures were frequent in accidental falls (p<0.001) (12).
We obtained ISS>12 in falling that were more than that in traffic accident. This is contrary to finding of Heidari et al. (12). This disagreement may be due to difference in lifestyle of people in different areas. Abnormal neurological examination occurred in 11.27% of patients. This is similar to Yousefzadeh et al. (2008) and Fakharian et al. findings (2003) (9,42).
In short, as many studies, we found that traffic accidents and falls from height are the most common cause of spinal injury. So, education and prevention through strict traffic laws and optimization of transport and improving people’s living and working conditions can be effective in reducing spinal damages. Our study was the first investigation that was designed to analyze spinal injury in Mazandaran. In a localized Sari environment, the present study showed a considerable amount of spinal cord injury which was mainly due to simultaneous associated injuries and associated trauma in subjects with spinal injury. The results of our study will be used to recommend policy makers, prioritize preventive measures, support the evaluation of interventions, and give guidance on the degree of injury and disability following specific types of TSF. Considering the high proportion of associated injuries in spinal injury, it is suggested that policy makers must provide preventive strategies to reduce the number and severity of spinal injury. Development of a nationwide SCI registry or observation system is essential to an understanding of the epidemiology, and the prevention of this costly health problem.
Conclusion
Motor vehicles accidents (MVAs) are the most common cause of spine and spinal cord injury in Mazandaran, a region in the north of Iran. Thoracolumbar fracture was more common in patients with MVAs. The incidence of SCI is high if ISS>12. Education and prevention through strict traffic laws can be effective on reducing damage to spine.
Recommendation
For rehabilitation period of treatment, we recommended designing a multicentric study in all cities of Mazandaran with five year period followed by long term follow-up of all patients discharged from hospital. Calculating cost of the first admission and rehabilitation period of patients with spinal injury is mandatory in future.
Funding
None.
Conflicts of Interest
The authors have no conflicts of interest.
References
Spinal cord injury (SCI) is a highly destructive situation (1) which is related to severe disability and death after trauma (2). Incidence of SCI is 12.1-57.8 cases per million (1) .The cost to the patient, their family and the health care system can be enormous (3).
In the US, spinal cord injury is the most costly traumatic condition. In a prospective population-based cohort study, Johnson et al. (4) reported that the costs for home care, services, and secondary medical complications reached almost $200,000 for each patient during the first two years after injury. The average cost of the first admission is approximately $95,203, with home modifications costing $8,203, medical services and equipment costing $7,866, and nurse and home care support costing $6,269 per year (5). An understanding of the epidemiology of SCI is essential for planning cost-effective care and for developing preventive strategies (6). Significant changes in SCI prevalence were observed among geographic locations, so these data are principal for local and regional health care economics (5). Rahimi-Movaghar et al. (2009) performed a population-based study to determine the prevalence of spine injury (SI) and spinal cord injury (SCI) in Tehran, Iran (7). The prevalence of traumatic SCI in Tehran ranged from 1.2 to 11.4 per 10,000 people.
Traumatic spine fracture (TSF) can occur as an isolated lesion or associated with other injuries such as to the spinal cord, head, extremities, and other organs injuries. Role of spine injury as a potential cause of disability and/or death is usually neglected. It commonly causes short-term disability (8), but may also result in long-term or even permament disability (9). Although the incidence of TSF increases in old population (5-8), it mostly involves young persons (10), which may increase the burden of this disease.
Although more than 80% of the world's population live in developing countries, little information is available regarding the epidemiology of SCI in these countries. The aim of the study was to determine regional epidemiology, demographics, mechanisms and severity of spine and spinal cord injury in a great area of north of Iran, Mazandaran.
Methods and Materials/Patients
Our cross-sectional study was performed on all patients with traumatic spine injury admitted to our hospital, the major trauma center in Mazandaran, an Iranian province, between January 2012 and November 2014.
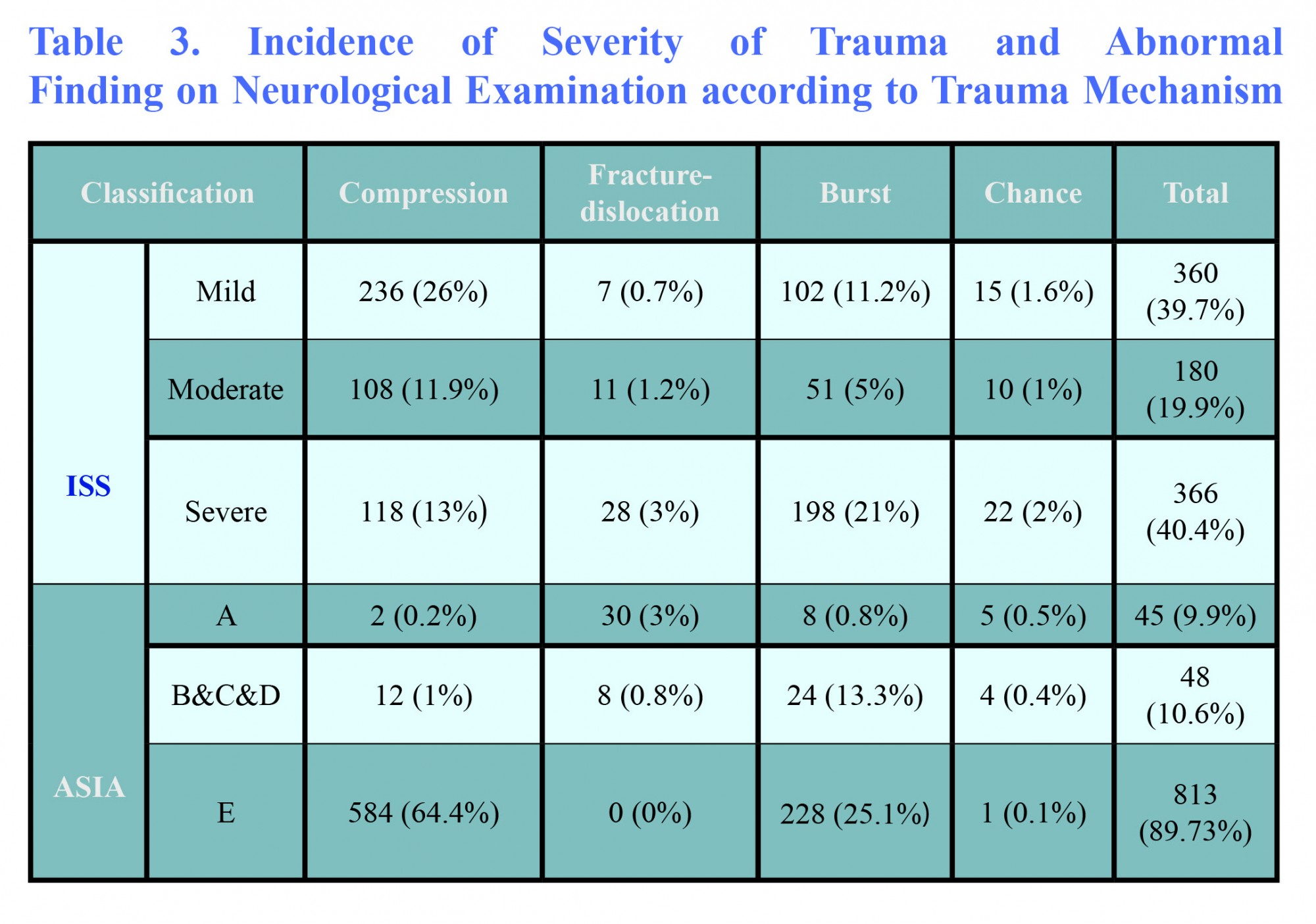
The demographic characteristics, mechanism of trauma, level and type of spinal fracture detected by radiologic imaging and MRI and CT scans, were obtained. We used the American Spinal Injury Association (ASIA) scale and Injury Severity Score (ISS) for classifying the severity of injury.
According to ASIA scale, patients were classified as (A: complete; B, C, D: incomplete; E: normal), and on the basis of ISS, they were categorized as (severe: > 12, moderate: 7-12, mild: < 7). All data were analyzed by SPSS.
Results
Total of 906 patients with traumatic spine injury (SI) were identified; 57.8% (n=523) of patients were male and 42.2% (n=383) were female. Male/female ratio was 1.37:1 (Table 1).
Sex Number Mean Age (Year ± SD)
Male 523 32.3±22.33
Female 383 38.6±26.11
Male/Female Ratio 1.37/1 -
The peak frequency of SI in males occurred in 25-44 year-old age group, and in females it took place in 45-65 year–old age group. Men were significantly younger than women (p=0.044).
Traffic accidents were the most common cause of spine injury (71.6%). The remaining ones were fall (26.5%) and other mechanisms (1.8%).
Traffic accidents tended to occur in younger age group, whereas falls tended to happen in older patients (38.5% in >64 year-olds) (p=0.004) (Figure 1).
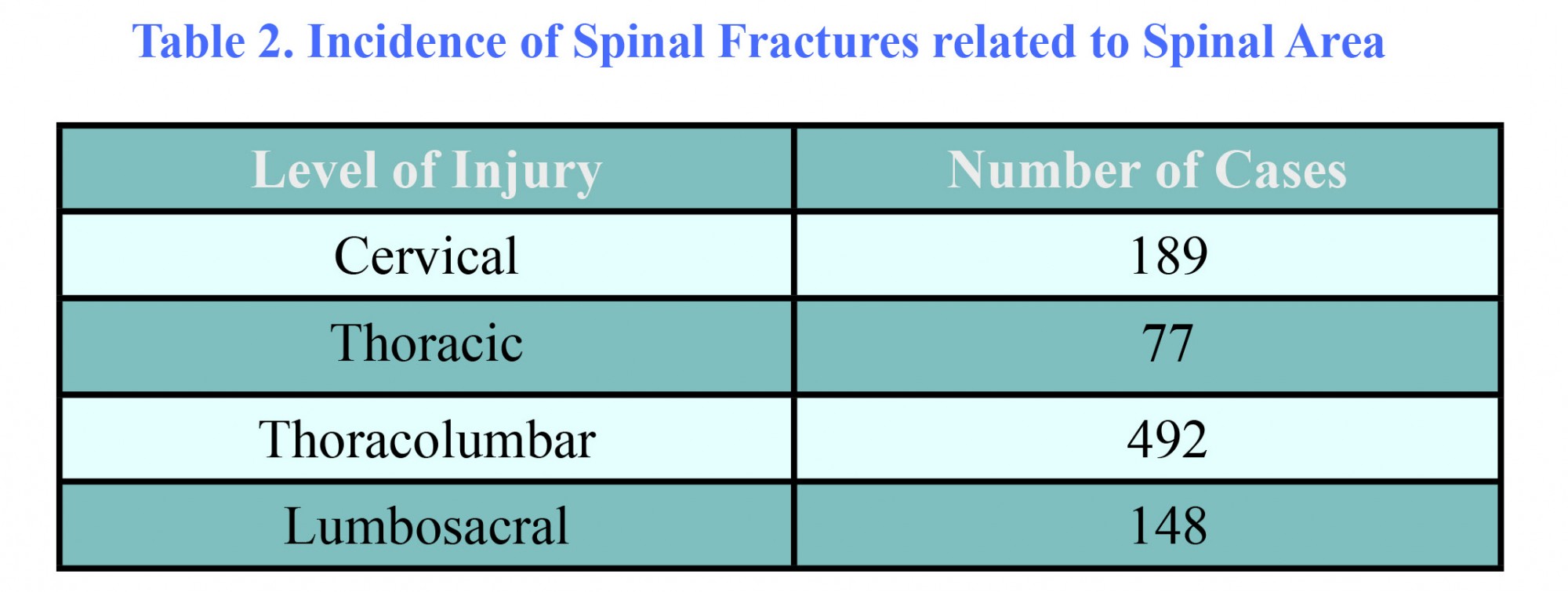
Thoracolumbar fractures were more common in patients with motor vehicle accidents (74.1%), while thoracic fractures were more frequent in fall patients (40%). Table 2 shows the incidence of spinal fractures from traumatic causes based on spinal area.
93 out of 906 patients with spinal trauma had abnormal finding on neurological examination (10.2%). 45 (4.9%) patients were classified as having ASIA A injuries. 48 (5.29%) patients had ASIA B,C,D (Table 3). 23 patients with complete spinal cord injury had tetraplegia, and 22 patients (48.8%) had paraplegia. 23 patients with complete spinal cord injuries (51%) had fracture or dislocation of cervical spine. Tetraplegia occurred in 12 (25%) patients with incomplete SCI, and paraplegia happened in 12 (25%) patients, and 24 (50%) of patients with incomplete SCI had no plegia. ISS>12 was seen in 43% of patients with thoracolumbar injuries, and 35% of patients with cervical injuries and 40% of cases with thoracic injuries. 36.2% of spinal fractures were caused by traffic accident injury, while 27.9% of them resulted from fall.
Discussion
At present, reporting on prevalence of spinal injury in Iran is conducted very little (4-7). The current prospective cross sectional study was performed on the SCI patients admitted at the major
trauma center in Mazandaran, an Iranian province from 2012 to 2014. According to our study confirmed by previous studies' reports, injuries in males were more than those in females (11-19).
Ning et al. (2010) did systematic review in Asia; they found that men were subject to higher risk of traumatic spinal cord injury (TSCI) than women (20). This difference may be caused by social expectations that men should support their family and men tend to do dangerous works to get more money. Peak of injury in males occur in 25-44 year-olds, and traffic accident was the most common cause of SCI in 25-44 year-olds. This finding is similar to Yousefzadeh et al. (2008) and Taghipour et al. (2005) and Fakharian et al results (2003) (9,11,21). In all countries, the highest incidences were reported in persons aged between 20 and 50 years (22). The average age in North America (23) was between 32 and 55.4 years, and in Europe (14-16,24,25) was between 37 and 47.9 years. Asian studies reported an average age between 26.8 and 56.6 years (20). These similar estimations in the world indicate that most cases of traumatic spine injury (TSI) are observed in adults because they are the most active members of society, and despite regional and demographic differences, these studies confirm worldwide tendency.
Traffic accidents are the most common cause of TSI in Europe (14,26-28), North America (29-32) and sub-Saharan Africa (33). In western Norway (34), falls were the most common cause. Ning et al. (2010) reported motor vehicle collisions (MVCs) and falls were the main causes of TSI in Asia and the latter has been increasing (20). In underdeveloped areas in Asia, motor vehicle usage is not as common as in North America and Europe (20). In China (35,36), there was a large group of old patients with degenerative cervical spine changes who were more exposed to a minor damage (e.g. a low-height fall), so the number of low-height falls-induced TSI gradually increased. Common cause in Bangladesh, (37,38) is falls, while carrying heavy loads on neck or back. Firearm wounds is a specific problem in Afghanistan (39), Jordan (40) and southeastern Turkey (41).Ning et al. (2010) did systematic review in Asia; they found that men were subject to higher risk of traumatic spinal cord injury (TSCI) than women (20). This difference may be caused by social expectations that men should support their family and men tend to do dangerous works to get more money. Peak of injury in males occur in 25-44 year-olds, and traffic accident was the most common cause of SCI in 25-44 year-olds. This finding is similar to Yousefzadeh et al. (2008) and Taghipour et al. (2005) and Fakharian et al results (2003) (9,11,21). In all countries, the highest incidences were reported in persons aged between 20 and 50 years (22). The average age in North America (23) was between 32 and 55.4 years, and in Europe (14-16,24,25) was between 37 and 47.9 years. Asian studies reported an average age between 26.8 and 56.6 years (20). These similar estimations in the world indicate that most cases of traumatic spine injury (TSI) are observed in adults because they are the most active members of society, and despite regional and demographic differences, these studies confirm worldwide tendency.
Variation of lifestyle in different countries and different regions of a country influence mechanism of trauma.
Yousefzadeh et al. (2008) showed thoracolumbar spine was common area for fracture (42). In our study, thoracolumbar spine was common involved area in traffic accidents, and thoracic spine was frequent site for falling. But Heidari et al. (2010) reported that cervical spine fractures were significantly common in road traffic accidents, and lumbar fractures were frequent in accidental falls (p<0.001) (12).
We obtained ISS>12 in falling that were more than that in traffic accident. This is contrary to finding of Heidari et al. (12). This disagreement may be due to difference in lifestyle of people in different areas. Abnormal neurological examination occurred in 11.27% of patients. This is similar to Yousefzadeh et al. (2008) and Fakharian et al. findings (2003) (9,42).
In short, as many studies, we found that traffic accidents and falls from height are the most common cause of spinal injury. So, education and prevention through strict traffic laws and optimization of transport and improving people’s living and working conditions can be effective in reducing spinal damages. Our study was the first investigation that was designed to analyze spinal injury in Mazandaran. In a localized Sari environment, the present study showed a considerable amount of spinal cord injury which was mainly due to simultaneous associated injuries and associated trauma in subjects with spinal injury. The results of our study will be used to recommend policy makers, prioritize preventive measures, support the evaluation of interventions, and give guidance on the degree of injury and disability following specific types of TSF. Considering the high proportion of associated injuries in spinal injury, it is suggested that policy makers must provide preventive strategies to reduce the number and severity of spinal injury. Development of a nationwide SCI registry or observation system is essential to an understanding of the epidemiology, and the prevention of this costly health problem.
Conclusion
Motor vehicles accidents (MVAs) are the most common cause of spine and spinal cord injury in Mazandaran, a region in the north of Iran. Thoracolumbar fracture was more common in patients with MVAs. The incidence of SCI is high if ISS>12. Education and prevention through strict traffic laws can be effective on reducing damage to spine.
Recommendation
For rehabilitation period of treatment, we recommended designing a multicentric study in all cities of Mazandaran with five year period followed by long term follow-up of all patients discharged from hospital. Calculating cost of the first admission and rehabilitation period of patients with spinal injury is mandatory in future.
Funding
None.
Conflicts of Interest
The authors have no conflicts of interest.
References
- Van den Berg ME, Castellote JM, Mahillo-Fernandez I, de Pedro-Cuesta J. Incidence of spinal cord injury worldwide: a systematic review. Neuroepidemiology. 2010;34(3):184-92.
- Flemming, K., R. Brown Jr, and H. Winn, Youmans Neurological Surgery. Youmans Neurological Surgery, 2004.
- Dryden DM, Saunders LD, Jacobs P, Schopflocher DP, Rowe BH, May LA, et al. Direct health care costs following traumatic spinal cord injury. Annals of Epidemiology. 2004;14(8):611-2.
- Wyndaele M, Wyndaele JJ. Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey?. Spinal cord. 2006;44(9):523-9.
- Pickelsimer E, Shiroma EJ, Wilson DA. Statewide investigation of medically attended adverse health conditions of persons with spinal cord injury. The journal of spinal cord medicine. 2010;33(3):221-31.
- Lee BB, Cripps RA, Fitzharris M, Wing PC. The global map for traumatic spinal cord injury epidemiology: update 2011, global incidence rate. Spinal cord. 2014;52(2):110-6.
- Rahimi-Movaghar V, Saadat S, Rasouli MR, Ganji S, Ghahramani M, Zarei MR, et al. Prevalence of spinal cord injury in Tehran, Iran. The journal of spinal cord medicine. 2009;32(4):428.
- Ackery A, Tator C, Krassioukov A. A global perspective on spinal cord injury epidemiology. Journal of neurotrauma. 2004;21(10):1355-70.
- Fakharian E, Fazel MR, Tabesh H, Nabavi Z. Incidence of mild head injury, management, and expenses in Kashan, 2003-2004. KAUMS Journal (FEYZ). 2007;11(3):63-7.
- Rasouli MR, Nouri M, Rahimi-Movaghar V. Spinal cord injuries from road traffic crashes in southeastern Iran. Chinese journal of traumatology= Zhonghua chuang shang za zhi/Chinese Medical Association. 2007;10(6):323-6.
- Chabok SY, Safaee M, Alizadeh A, Dafchahi MA, Taghinnejadi O, Koochakinejad L. Epidemiology of traumatic spinal injury: a descriptive study. Acta Medica Iranica. 2010;48(5):308.
- Pedram H, Reza ZM, Reza RM, Vaccaro AR, Vafa RM. Spinal fractures resulting from traumatic injuries. Chinese Journal of Traumatology (English Edition). 2010;13(1):3-9.
- Quinones PM, Nassal M, AlBader KI, Al Muraikhi AE, Al Kahlout SR. Traumatic spinal cord injury in Qatar: an epidemiological study. Middle East J Emergency Med. 2002;2(1):35-40.
- Knutsdottir S, Thorisdottir H, Sigvaldason K, Jónsson H, Björnsson A, Ingvarsson P. Epidemiology of traumatic spinal cord injuries in Iceland from 1975 to 2009. Spinal cord. 2012;50(2):123-6.
- Amin A, Bernard J, Nadarajah R, Davies N, Gow F, Tucker S. Spinal injuries admitted to a specialist centre over a 5-year period: a study to evaluate delayed admission. Spinal Cord. 2005;43(7):434-7.
- O'Connor RJ, Murray PC. Review of spinal cord injuries in Ireland. Spinal Cord. 2006;44(7):445-8.
- O’Connor, P.J. Forecasting of spinal cord injury annual case numbers in Australia. Archives of physical medicine and rehabilitation, 2005;86(1):48-51.
- Obalum DC, Giwa SO, Adekoya-Cole TO, Enweluzo GO. Profile of spinal injuries in Lagos, Nigeria. Spinal Cord. 2009;47(2):134-7.
- Maharaj, J.C. Epidemiology of spinal cord paralysis in Fiji. 1985-1994. Spinal Cord, 1996;34(9):549-559.
- Ning GZ, Wu Q, Li YL, Feng SQ. Epidemiology of traumatic spinal cord injury in Asia: a systematic review. The journal of spinal cord medicine. 2012 ;35(4):229-39.
- Taghippor M, Sherafat Kazemzadeh E. Column and Spinal Cord Injuries in Shiraz Nemazi Hospital, an Epidemiological Study. Armaghane danesh. 2006 ;10(4):55-62.
- Nobunaga AI, Go BK, Karunas RB. Recent demographic and injury trends in people served by the Model Spinal Cord Injury Care Systems. Archives of physical medicine and rehabilitation. 1999;80(11):1372-82.
- Calancie B, Molano MR, Broton JG. Epidemiology and demography of acute spinal cord injury in a large urban setting. The journal of spinal cord medicine. 2004;28(2):92-6.
- Dahlberg A, Kotila M, Leppänen P, Kautiainen H, Alaranta H. Prevalence of spinal cord injury in Helsinki. Spinal Cord. 2005;43(1):47-50.
- Divanoglou A, Levi R. Incidence of traumatic spinal cord injury in Thessaloniki, Greece and Stockholm, Sweden: a prospective population-based study. Spinal Cord. 2009;47(11):796-801.
- Martins F, Freitas F, Martins L, Dartigues JF, Barat M. Spinal cord injuries ą Epidemiology in Portugal's central region. Spinal Cord. 1998;36(574):578.
- Silberstein B, Rabinovich S. Epidemiology of spinal cord injuries in Novosibirsk, Russia. Spinal Cord. 1995;33(6):322-5.
- Van Asbeck FW, Post MW, Pangalila RF. An epidemiological description of spinal cord injuries in The Netherlands in 1994. Spinal cord. 2000;38(7):420-4.
- Dryden DM, Saunders LD, Rowe BH, May LA, Yiannakoulias N, Svenson LW, Schopflocher DP, et al. The epidemiology of traumatic spinal cord injury in Alberta, Canada. The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques. 2003;30(2):113-21.
- Pickett GE, Campos-Benitez M, Keller JL, Duggal N. Epidemiology of traumatic spinal cord injury in Canada. Spine. 2006;31(7):799-805.
- Surkin J, Gilbert BJ, Harkey III HL, Sniezek J, Currier M. Spinal cord injury in Mississippi: findings and evaluation, 1992–1994. Spine. 2000;25(6):716-21.
- Pirouzmand, F. Epidemiological trends of spine and spinal cord injuries in the largest Canadian adult trauma center from 1986 to 2006: clinical article. Journal of neurosurgery: Spine, 2010;12(2):131-140.
- Draulans N, Kiekens C, Roels E, Peers K. Etiology of spinal cord injuries in Sub-Saharan Africa. Spinal Cord. 2011;49(12):1148-54.
- Hagen EM, Eide GE, Rekand T, Gilhus NE, Gronning M. A 50-year follow-up of the incidence of traumatic spinal cord injuries in Western Norway. Spinal Cord. 2010;48(4):313-8.
- Ning GZ, Yu TQ, Feng SQ, Zhou XH, Ban DX, Liu Y, et al. Epidemiology of traumatic spinal cord injury in Tianjin, China. Spinal Cord. 2011;49(3):386-90.
- Feng HY, Ning GZ, Feng SQ, Yu TQ, Zhou HX. Epidemiological profile of 239 traumatic spinal cord injury cases over a period of 12 years in Tianjin, China. The journal of spinal cord medicine. 2011;34(4):388-94.
- Hoque MF, Grangeon C, Reed K. Spinal cord lesions in Bangladesh: an epidemiological study 1994–1995. Spinal cord. 1999;37(12).
- Islam MS, Hafez MA, Akter M. Characterization of spinal cord lesion in patients attending a specialized rehabilitation center in Bangladesh. Spinal cord. 2011;49(7):783-6.
- Deconinck, H., The health condition of spinal cord injuries in two Afghan towns. Spinal Cord, 2003;41(5):303-309.
- Otom AS, Doughan AM, Kawar JS, Hattar EZ. Traumatic spinal cord injuries in Jordan–an epidemiological study. Spinal Cord. 1997;35(4).
- Karamehmetoglu SS, Nas K, Karacan I, Sarac AJ, Koyuncu H, Ataoglu S, et al. Traumatic spinal cord injuries in southeast Turkey: an epidemiological study. Spinal Cord. 1997;35(8):531-3.
- Yousef zade Chabok SH, Safayi M, Hemati H, Mohammadi HA, Shabani S. Epidemiology of Head Injury In Patients Who Were Reffered To Poorsina Hospital. Journal of Guilan University of Medical Sciences. 2008;16(64):112-9.
Type of Study: Research |
Subject:
Gamma Knife Radiosurgery
References
1. Van den Berg ME, Castellote JM, Mahillo-Fernandez I, de Pedro-Cuesta J. Incidence of spinal cord injury worldwide: a systematic review. Neuroepidemiology. 2010;34(3):184-92. [DOI:10.1159/000279335] [PMID]
2. Flemming, K., R. Brown Jr, and H. Winn, Youmans Neurological Surgery. Youmans Neurological Surgery, 2004.
3. Dryden DM, Saunders LD, Jacobs P, Schopflocher DP, Rowe BH, May LA, et al. Direct health care costs following traumatic spinal cord injury. Annals of Epidemiology. 2004;14(8):611-2. [DOI:10.1016/j.annepidem.2004.07.055]
4. Wyndaele M, Wyndaele JJ. Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey?. Spinal cord. 2006;44(9):523-9. [DOI:10.1038/sj.sc.3101893] [PMID]
5. Pickelsimer E, Shiroma EJ, Wilson DA. Statewide investigation of medically attended adverse health conditions of persons with spinal cord injury. The journal of spinal cord medicine. 2010;33(3):221-31. [DOI:10.1080/10790268.2010.11689699] [PMID] [PMCID]
6. Lee BB, Cripps RA, Fitzharris M, Wing PC. The global map for traumatic spinal cord injury epidemiology: update 2011, global incidence rate. Spinal cord. 2014;52(2):110-6. [DOI:10.1038/sc.2012.158] [PMID]
7. Rahimi-Movaghar V, Saadat S, Rasouli MR, Ganji S, Ghahramani M, Zarei MR, et al. Prevalence of spinal cord injury in Tehran, Iran. The journal of spinal cord medicine. 2009;32(4):428. [DOI:10.1080/10790268.2009.11754572] [PMID] [PMCID]
8. Ackery A, Tator C, Krassioukov A. A global perspective on spinal cord injury epidemiology. Journal of neurotrauma. 2004;21(10):1355-70. [DOI:10.1089/neu.2004.21.1355] [PMID]
9. Fakharian E, Fazel MR, Tabesh H, Nabavi Z. Incidence of mild head injury, management, and expenses in Kashan, 2003-2004. KAUMS Journal (FEYZ). 2007;11(3):63-7.
10. Rasouli MR, Nouri M, Rahimi-Movaghar V. Spinal cord injuries from road traffic crashes in southeastern Iran. Chinese journal of traumatology= Zhonghua chuang shang za zhi/Chinese Medical Association. 2007;10(6):323-6.
11. Chabok SY, Safaee M, Alizadeh A, Dafchahi MA, Taghinnejadi O, Koochakinejad L. Epidemiology of traumatic spinal injury: a descriptive study. Acta Medica Iranica. 2010;48(5):308.
12. Pedram H, Reza ZM, Reza RM, Vaccaro AR, Vafa RM. Spinal fractures resulting from traumatic injuries. Chinese Journal of Traumatology (English Edition). 2010;13(1):3-9. [PMID]
13. Quinones PM, Nassal M, AlBader KI, Al Muraikhi AE, Al Kahlout SR. Traumatic spinal cord injury in Qatar: an epidemiological study. Middle East J Emergency Med. 2002;2(1):35-40.
14. Knutsdottir S, Thorisdottir H, Sigvaldason K, Jónsson H, Björnsson A, Ingvarsson P. Epidemiology of traumatic spinal cord injuries in Iceland from 1975 to 2009. Spinal cord. 2012;50(2):123-6. [DOI:10.1038/sc.2011.105] [PMID]
15. Amin A, Bernard J, Nadarajah R, Davies N, Gow F, Tucker S. Spinal injuries admitted to a specialist centre over a 5-year period: a study to evaluate delayed admission. Spinal Cord. 2005;43(7):434-7. [DOI:10.1038/sj.sc.3101734] [PMID]
16. O'Connor RJ, Murray PC. Review of spinal cord injuries in Ireland. Spinal Cord. 2006;44(7):445-8. [DOI:10.1038/sj.sc.3101856] [PMID]
17. O'Connor, P.J. Forecasting of spinal cord injury annual case numbers in Australia. Archives of physical medicine and rehabilitation, 2005;86(1):48-51. [DOI:10.1016/j.apmr.2004.07.346] [PMID]
18. Obalum DC, Giwa SO, Adekoya-Cole TO, Enweluzo GO. Profile of spinal injuries in Lagos, Nigeria. Spinal Cord. 2009;47(2):134-7. [DOI:10.1038/sc.2008.93] [PMID]
19. Maharaj, J.C. Epidemiology of spinal cord paralysis in Fiji. 1985-1994. Spinal Cord, 1996;34(9):549-559. [DOI:10.1038/sc.1996.99] [PMID]
20. Ning GZ, Wu Q, Li YL, Feng SQ. Epidemiology of traumatic spinal cord injury in Asia: a systematic review. The journal of spinal cord medicine. 2012 ;35(4):229-39. [DOI:10.1179/2045772312Y.0000000021] [PMID] [PMCID]
21. Taghippor M, Sherafat Kazemzadeh E. Column and Spinal Cord Injuries in Shiraz Nemazi Hospital, an Epidemiological Study. Armaghane danesh. 2006 ;10(4):55-62.
22. Nobunaga AI, Go BK, Karunas RB. Recent demographic and injury trends in people served by the Model Spinal Cord Injury Care Systems. Archives of physical medicine and rehabilitation. 1999;80(11):1372-82. [DOI:10.1016/S0003-9993(99)90247-2]
23. Calancie B, Molano MR, Broton JG. Epidemiology and demography of acute spinal cord injury in a large urban setting. The journal of spinal cord medicine. 2004;28(2):92-6. [DOI:10.1080/10790268.2005.11753804]
24. Dahlberg A, Kotila M, Leppänen P, Kautiainen H, Alaranta H. Prevalence of spinal cord injury in Helsinki. Spinal Cord. 2005;43(1):47-50. [DOI:10.1038/sj.sc.3101616] [PMID]
25. Divanoglou A, Levi R. Incidence of traumatic spinal cord injury in Thessaloniki, Greece and Stockholm, Sweden: a prospective population-based study. Spinal Cord. 2009;47(11):796-801. [DOI:10.1038/sc.2009.28] [PMID]
26. Martins F, Freitas F, Martins L, Dartigues JF, Barat M. Spinal cord injuries ą Epidemiology in Portugal's central region. Spinal Cord. 1998;36(574):578. [DOI:10.1038/sj.sc.3100657]
27. Silberstein B, Rabinovich S. Epidemiology of spinal cord injuries in Novosibirsk, Russia. Spinal Cord. 1995;33(6):322-5. [DOI:10.1038/sc.1995.72] [PMID]
28. Van Asbeck FW, Post MW, Pangalila RF. An epidemiological description of spinal cord injuries in The Netherlands in 1994. Spinal cord. 2000;38(7):420-4. [DOI:10.1038/sj.sc.3101003] [PMID]
29. Dryden DM, Saunders LD, Rowe BH, May LA, Yiannakoulias N, Svenson LW, Schopflocher DP, et al. The epidemiology of traumatic spinal cord injury in Alberta, Canada. The Canadian journal of neurological sciences. Le journal canadien des sciences neurologiques. 2003;30(2):113-21.
30. Pickett GE, Campos-Benitez M, Keller JL, Duggal N. Epidemiology of traumatic spinal cord injury in Canada. Spine. 2006;31(7):799-805. [DOI:10.1097/01.brs.0000207258.80129.03] [PMID]
31. Surkin J, Gilbert BJ, Harkey III HL, Sniezek J, Currier M. Spinal cord injury in Mississippi: findings and evaluation, 1992–1994. Spine. 2000;25(6):716-21. [DOI:10.1097/00007632-200003150-00011] [PMID]
32. Pirouzmand, F. Epidemiological trends of spine and spinal cord injuries in the largest Canadian adult trauma center from 1986 to 2006: clinical article. Journal of neurosurgery: Spine, 2010;12(2):131-140. [DOI:10.3171/2009.9.SPINE0943] [PMID]
33. Draulans N, Kiekens C, Roels E, Peers K. Etiology of spinal cord injuries in Sub-Saharan Africa. Spinal Cord. 2011;49(12):1148-54. [DOI:10.1038/sc.2011.93] [PMID]
34. Hagen EM, Eide GE, Rekand T, Gilhus NE, Gronning M. A 50-year follow-up of the incidence of traumatic spinal cord injuries in Western Norway. Spinal Cord. 2010;48(4):313-8. [DOI:10.1038/sc.2009.133] [PMID]
35. Ning GZ, Yu TQ, Feng SQ, Zhou XH, Ban DX, Liu Y, et al. Epidemiology of traumatic spinal cord injury in Tianjin, China. Spinal Cord. 2011;49(3):386-90. [DOI:10.1038/sc.2010.130] [PMID]
36. Feng HY, Ning GZ, Feng SQ, Yu TQ, Zhou HX. Epidemiological profile of 239 traumatic spinal cord injury cases over a period of 12 years in Tianjin, China. The journal of spinal cord medicine. 2011;34(4):388-94. [DOI:10.1179/2045772311Y.0000000017] [PMID] [PMCID]
37. Hoque MF, Grangeon C, Reed K. Spinal cord lesions in Bangladesh: an epidemiological study 1994–1995. Spinal cord. 1999;37(12). [DOI:10.1038/sj.sc.3100938] [PMID]
38. Islam MS, Hafez MA, Akter M. Characterization of spinal cord lesion in patients attending a specialized rehabilitation center in Bangladesh. Spinal cord. 2011;49(7):783-6. [DOI:10.1038/sc.2011.36] [PMID]
39. Deconinck, H., The health condition of spinal cord injuries in two Afghan towns. Spinal Cord, 2003;41(5):303-309. [DOI:10.1038/sj.sc.3101443] [PMID]
40. Otom AS, Doughan AM, Kawar JS, Hattar EZ. Traumatic spinal cord injuries in Jordan–an epidemiological study. Spinal Cord. 1997;35(4). [DOI:10.1038/sj.sc.3100402] [PMID]
41. Karamehmetoglu SS, Nas K, Karacan I, Sarac AJ, Koyuncu H, Ataoglu S, et al. Traumatic spinal cord injuries in southeast Turkey: an epidemiological study. Spinal Cord. 1997;35(8):531-3. [DOI:10.1038/sj.sc.3100404] [PMID]
42. Yousef zade Chabok SH, Safayi M, Hemati H, Mohammadi HA, Shabani S. Epidemiology of Head Injury In Patients Who Were Reffered To Poorsina Hospital. Journal of Guilan University of Medical Sciences. 2008;16(64):112-9.
| Rights and Permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
