Sun, Jul 13, 2025
Volume 4, Issue 3 (Summer 2018)
Iran J Neurosurg 2018, 4(3): 179-188 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ghadarjani S, Alijani B, Naseri A, Hamzei A. Dermoid Cysts of Conus Medullaris. Iran J Neurosurg 2018; 4 (3) :179-188
URL: http://irjns.org/article-1-134-en.html
URL: http://irjns.org/article-1-134-en.html



1- Assistant Professor of Neurosurgery, Department of Neurosurgery, Poursina Hospital, Guilan University of Medical Sciences, Guilan, Iran , shervin.gh2@gmail.com
2- Associate Professor of Neurosurgery, Department of Neurosurgery, Poursina Hospital, Guilan University of Medical Sciences, Guilan, Iran
3- Resident of Neurosurgery, Department of Neurosurgery, Poursina Hospital, Guilan University of Medical Sciences, Guilan, Iran
2- Associate Professor of Neurosurgery, Department of Neurosurgery, Poursina Hospital, Guilan University of Medical Sciences, Guilan, Iran
3- Resident of Neurosurgery, Department of Neurosurgery, Poursina Hospital, Guilan University of Medical Sciences, Guilan, Iran
Full Text [PDF 867 kb]
(2738 Downloads)
| Abstract (HTML) (4931 Views)




Full Text: (2628 Views)
Highlights
• Spinal dermoid cysts are uncommon and benign lesions, resulting from the inclusion of epithelial tissue within the neural groove during embryonic development.
• They are most often located in the lumbosacral region and cauda equina.
• Although benign and slow growing, they may rupture causing high morbidity and mortality.
• Surgical excision is the treatment of choice, resulting in improvement or stabilization of the patients’ symptoms.
Plain Language Summary
A dermoid cyst is a saclike growth that is present since birth. It contains structures such as hair, fluid, teeth, or skin glands. Dermoid cysts grow slowly and are not tender unless ruptured. They usually occur on the face, inside the skull, or spine. A sinus tract, which is a narrow connection from a deep pit in the skin, usually connects these very rare cysts to the skin surface, thus becomes a source of infection. Removal of the cyst is often incomplete, but the outcome is usually excellent..
1. Background and Importance
ermoid cysts are a rare lesions in the spinal canal with the prevalence rate of <1% in spinal tumors [1]. This lesion arise from ectopic ectodermal tissue during the embryonic development of central nervous system [2]. Dermoid cysts are benign lesions usually observed in the lumbosacral region of the spinal canal [3] and are often associated with congenital dermal sinus tracts and spinal dysraphism [4]. These lesionsare often present during the first and second decades of life; and are usually extramedullary intradural lesions [5]. Clinical signs and symptoms due to their compressive effect, which the irritation and compression of adjacent neural elements [6]. The rupture of this lesion can be associated with a high rate of morbidity and mortality [7]. We report a case of intra- and extra-medullaris dermoid cyst of conus medullaris with dysraphism who underwent subtotal resection surgery without complications.
2. Case Presentation
A 37-year-old man with progressive paralysis in distal part of the left lower limb presented to our clinic. His weakness aggravated since 2 months before admission to the hospital. He reported limitation in the dorsi- and plantar flexion of his left lower limb. The patient reported no lumbar pain or lower limb radiculopathy pain. The sphincter dysfunction was also not mentioned. He had no history of trauma. Physical examination revealed generalized atrophy in the lower limbs. The proximal, and distal left lower limb force were represented in sites M5 and M2, respectively. Positive upper motor neuron signs like increased deep tendon reflexes were evident in lower limbs. The sensory dysfunction or its level was not determined.
• Spinal dermoid cysts are uncommon and benign lesions, resulting from the inclusion of epithelial tissue within the neural groove during embryonic development.
• They are most often located in the lumbosacral region and cauda equina.
• Although benign and slow growing, they may rupture causing high morbidity and mortality.
• Surgical excision is the treatment of choice, resulting in improvement or stabilization of the patients’ symptoms.
Plain Language Summary
A dermoid cyst is a saclike growth that is present since birth. It contains structures such as hair, fluid, teeth, or skin glands. Dermoid cysts grow slowly and are not tender unless ruptured. They usually occur on the face, inside the skull, or spine. A sinus tract, which is a narrow connection from a deep pit in the skin, usually connects these very rare cysts to the skin surface, thus becomes a source of infection. Removal of the cyst is often incomplete, but the outcome is usually excellent..
1. Background and Importance
ermoid cysts are a rare lesions in the spinal canal with the prevalence rate of <1% in spinal tumors [1]. This lesion arise from ectopic ectodermal tissue during the embryonic development of central nervous system [2]. Dermoid cysts are benign lesions usually observed in the lumbosacral region of the spinal canal [3] and are often associated with congenital dermal sinus tracts and spinal dysraphism [4]. These lesionsare often present during the first and second decades of life; and are usually extramedullary intradural lesions [5]. Clinical signs and symptoms due to their compressive effect, which the irritation and compression of adjacent neural elements [6]. The rupture of this lesion can be associated with a high rate of morbidity and mortality [7]. We report a case of intra- and extra-medullaris dermoid cyst of conus medullaris with dysraphism who underwent subtotal resection surgery without complications.
2. Case Presentation
A 37-year-old man with progressive paralysis in distal part of the left lower limb presented to our clinic. His weakness aggravated since 2 months before admission to the hospital. He reported limitation in the dorsi- and plantar flexion of his left lower limb. The patient reported no lumbar pain or lower limb radiculopathy pain. The sphincter dysfunction was also not mentioned. He had no history of trauma. Physical examination revealed generalized atrophy in the lower limbs. The proximal, and distal left lower limb force were represented in sites M5 and M2, respectively. Positive upper motor neuron signs like increased deep tendon reflexes were evident in lower limbs. The sensory dysfunction or its level was not determined.
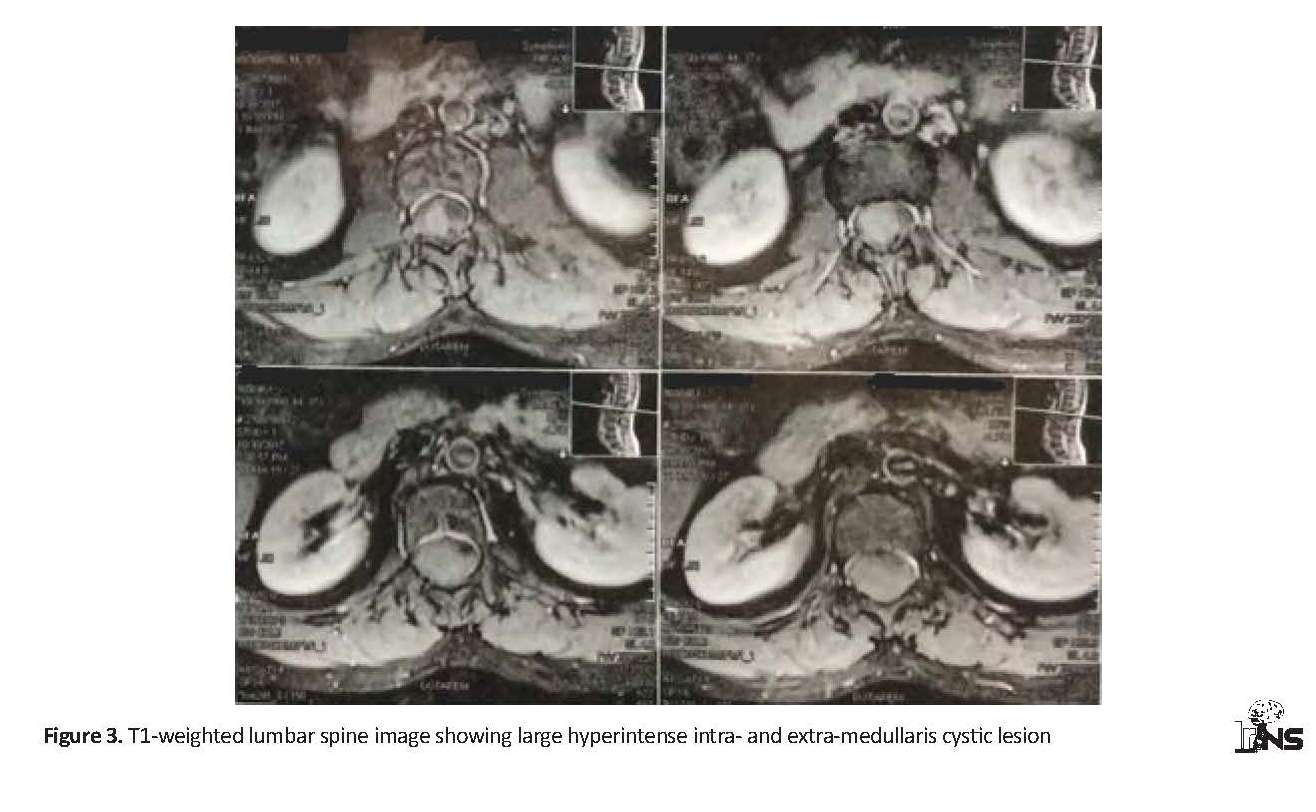
The lumbosacral plain radiography demonstrated dysraphism at L5 vertebra. The Magnetic Resonance Imaging (MRI) of lumbar spine, as a choice of modality, has revealed a large well-defined sausage-shaped lesion, a multilobular cyst, and the heterogeneous contrast enhancement of an intra- and extra-medullary lesions in the conus medullaris region, extending from T12 to L3 vertebral levels. It was hypointense on the T2-weighted images and hyperintense on T1-weighted images. Hypointensity on the T2-weighted indicated this lesion is not a lipoma. The lesion was not enhancing or rim-enhancing after the administration of gadolinium contrast. Therefore, the absence of rim enhancing can also exclude abscess (Figures 1, 2, 3). The differential diagnosis of this lesion includes teratoma, epidermoid cyst, lipoma or other lesions in this region, like myxopapillary ependymoma.
The patient underwent surgery under general anesthesia. During the surgery, we performed laminectomy from T12 to L3 without facetectomy to maintain stability. Then, the bulging of dura was observed. Durotomy was performed in midline, a large cyst was observed, laterally pushing cauda equina nerve roots along spinal cord. Myelotomy was performed in midline and dermoid cyst resection started; then, its capsule was opened and complete removal was conducted (Figure 3). It consisted of light brown pasty material and hair; it was removed and referred for histopathology (Figure 4). Subtotal microsurgical resection was performed on the lesion.
The result of histopathological examination confirmed the dermoid cyst, as well. The specimen consisted of plenty cellular keratin debris with the occasional fragments of keratinized squamous epithelium. Several hair fragments, a diagnostic finding of a dermoid cyst, were also identified (Figure 5). Postoperative examination detected no new motor deficits and there was no bladder or intestinal dysfunction Figure 4. An intraoperative photograph showing conus dermoid cyst with a bright yellow gelatinous material and hair after dural opening
3. Discussion
Dermoid cysts are rare lesions in the central nervous system accounting for approximately 1.1% of intra-spinal lesions [1]. These lesions are benign and usually located in the lumbosacral region. They arise from the inclusion of ectopic embryonic rests of ectoderm within the spinal canal at the time of neural tube closure in embryo [2, 3].
Based on the theory of embryological malformation, during the neural groove closure, the ectodermal folds are trapped under the fusion line; therefore, this is not a true neoplasm [8, 9]. Although these lesions developed from an embryonic period, due to their slow-growth, do not present symptoms until adulthood [5]. They may be associated with the other forms of dysraphism and a dorsal dermal sinus can be observed in about 20% of all cases [4]. Imaging modality of choice is MRI. The manifestation of dermoid cyst is a unilocular or multilocular cystic with different intensity due to different cystic contents. The main contents, namely liquid and fat, are detectable in MRI as hypo-intensities and hyper-intensities in T2- and T1-weighted MR imaging, respectively.
3. Discussion
Dermoid cysts are rare lesions in the central nervous system accounting for approximately 1.1% of intra-spinal lesions [1]. These lesions are benign and usually located in the lumbosacral region. They arise from the inclusion of ectopic embryonic rests of ectoderm within the spinal canal at the time of neural tube closure in embryo [2, 3].
Based on the theory of embryological malformation, during the neural groove closure, the ectodermal folds are trapped under the fusion line; therefore, this is not a true neoplasm [8, 9]. Although these lesions developed from an embryonic period, due to their slow-growth, do not present symptoms until adulthood [5]. They may be associated with the other forms of dysraphism and a dorsal dermal sinus can be observed in about 20% of all cases [4]. Imaging modality of choice is MRI. The manifestation of dermoid cyst is a unilocular or multilocular cystic with different intensity due to different cystic contents. The main contents, namely liquid and fat, are detectable in MRI as hypo-intensities and hyper-intensities in T2- and T1-weighted MR imaging, respectively.
Various abnormalities might be present with existing dermoid cyst, e.g. hypertrichosis, myelomeningocele and dermal sinus tract or mixture of these [10, 11]. The histological distinction from epidermoid cyst arises from the dermal appendages like sebaceous sweat glands , hair and hair follicles characteristic for dermoid cysts [9]. The mortality and morbidity risks in dermoid cyst depends on the cyst wall to be intact. If it ruptures, a high degree of poor outcome is associated with lipid droplets scattered throughout the spinal cord [7].
A Rupture may occur spontaneously or following traumatic or iatrogenic incidences. It could remain asymptomatic or lead to headache and nausea, vomiting, meningismus or aggravated neurological condition, or coma. These symptoms are assumed to arise from chemical or aseptic arachnoiditis or meningitis secondary to the leakage of lipid and proteinaceus material in the subarachnoid space [10].
Subtotal resection is used for the treatment of intra- and extra-medullary spinal cord dermoid cyst, because the cyst capsule is frequently tightly adhered to the neural structure, leading to even more neurological deficits during forced total resection. Chemotherapy and radiotherapy are not used to treat this lesion. Steroids are useful in the treatment of meningitis caused by rupture [12]. In our reported case, the patient received treatment after subtotal resection, leading to desirable clinical outcomes.
4. Conclusion
Treatment of dermoid cysts of conus medullaris are challenging for physicians. Symptoms are usually chronic neurological deficits due to compression of nerves or acute due to cyst rupture. Subtotal resection is used for the treatment of these lesions.
Ethical Considerations
Compliance with ethical guidelines
All personal details of the patient were kept confidential. Moreover, the patient's name has been removed from the relevant images.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed in designing, running, and writing all parts of the research.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
We thank Dr. Beykian for his assistance in histopathological investigation.
References
Manno NJ, Uihlein A, Kernohan JW. Intraspinalepidermoids. Journal of Neurosurgery. 1962; 19:754-765. [DOI:10.3171/jns.1962.19.9.0754] [PMID]
Netsky MG. Epidermoid tumors: Review of the literature. Surgical Neurology. 1988; 29(6):477-83. [DOI:10.1016/0090-3019(88)90144-9]
Najjar MW, Kusske JA, Hasso AN. Dorsal intramedullary dermoids. Neurosurgical Review. 2005; 28(4):320-5. [DOI:10.1007/s10143-005-0382-9] [PMID]
Shubha AM, Mohanty S, Das K, Garg I. Congenital inclusion tumors in the spinal dysraphism. The Indian Journal of Pediatrics. 2010; 77(2):167-70. [DOI:10.1007/s12098-009-0290-z] [PMID]
Lunardi P, Missori P, Gagliardi FM, Fortuna A. Long-term results of the surgical treatment of spinal dermoid and epidermoid tumors. Neurosurgery. 1989; 25(6):860-4. [DOI:10.1227/00006123-198912000-00002] [PMID]
Do-Dai DD, Brooks MK, Goldkamp A, Erbay S, Bhadelia RA. Magnetic resonance imaging of intramedullary spinal cord lesions: A pictorial review. Current Problems in Diagnostic Radiology. 2010; 39(4):160-85. [DOI:10.1067/j.cpradiol.2009.05.004]
Altay H, Kitis Ö, Çalli C, Yünten N. A spinal dermoid tumor that ruptured into the subarachnoidal space and syrinx cavity. Diagnostic and Interventional Radiology. 2006; 12(4):171-3. [PMID]
Patankar AP, Sheth JH. Dermoid cyst: A rare intramedullary inclusion cyst. Asian journal of neurosurgery. 2012; 7(2):81-3. [DOI:10.4103/1793-5482.98651] [PMID] [PMCID]
De Maio PN, Mikulis DJ, Kiehl TR, Guha A. AIRP best cases in radiologic-pathologic correlation: Spinal Conus dermoid cyst with lipid dissemination. Radiographics. 2012; 32(4):1215-21. [DOI:10.1148/rg.324115018] [PMID]
Calabrò F, Capellini C, Jinkins JR. Rupture of spinal dermoid tumors with spread of fatty droplets in the cerebrospinal fluid pathways. Neuroradiology. 2000; 42(8):572-9. [DOI:10.1007/s002340000345] [PMID]
Cha JG, Paik SH, Park JS, Park SJ, Kim DH, Lee HK. Ruptured spinal dermoid cyst with disseminated intracranial fat droplets. The British Journal of Radiology. 2006; 79(938):167-9. [DOI:10.1259/bjr/17232685] [PMID]
Winn HR. Youmans neurological surgery. Philadelphia: Elsevier; 2004.
A Rupture may occur spontaneously or following traumatic or iatrogenic incidences. It could remain asymptomatic or lead to headache and nausea, vomiting, meningismus or aggravated neurological condition, or coma. These symptoms are assumed to arise from chemical or aseptic arachnoiditis or meningitis secondary to the leakage of lipid and proteinaceus material in the subarachnoid space [10].
Subtotal resection is used for the treatment of intra- and extra-medullary spinal cord dermoid cyst, because the cyst capsule is frequently tightly adhered to the neural structure, leading to even more neurological deficits during forced total resection. Chemotherapy and radiotherapy are not used to treat this lesion. Steroids are useful in the treatment of meningitis caused by rupture [12]. In our reported case, the patient received treatment after subtotal resection, leading to desirable clinical outcomes.
4. Conclusion
Treatment of dermoid cysts of conus medullaris are challenging for physicians. Symptoms are usually chronic neurological deficits due to compression of nerves or acute due to cyst rupture. Subtotal resection is used for the treatment of these lesions.
Ethical Considerations
Compliance with ethical guidelines
All personal details of the patient were kept confidential. Moreover, the patient's name has been removed from the relevant images.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed in designing, running, and writing all parts of the research.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
We thank Dr. Beykian for his assistance in histopathological investigation.
References
Manno NJ, Uihlein A, Kernohan JW. Intraspinalepidermoids. Journal of Neurosurgery. 1962; 19:754-765. [DOI:10.3171/jns.1962.19.9.0754] [PMID]
Netsky MG. Epidermoid tumors: Review of the literature. Surgical Neurology. 1988; 29(6):477-83. [DOI:10.1016/0090-3019(88)90144-9]
Najjar MW, Kusske JA, Hasso AN. Dorsal intramedullary dermoids. Neurosurgical Review. 2005; 28(4):320-5. [DOI:10.1007/s10143-005-0382-9] [PMID]
Shubha AM, Mohanty S, Das K, Garg I. Congenital inclusion tumors in the spinal dysraphism. The Indian Journal of Pediatrics. 2010; 77(2):167-70. [DOI:10.1007/s12098-009-0290-z] [PMID]
Lunardi P, Missori P, Gagliardi FM, Fortuna A. Long-term results of the surgical treatment of spinal dermoid and epidermoid tumors. Neurosurgery. 1989; 25(6):860-4. [DOI:10.1227/00006123-198912000-00002] [PMID]
Do-Dai DD, Brooks MK, Goldkamp A, Erbay S, Bhadelia RA. Magnetic resonance imaging of intramedullary spinal cord lesions: A pictorial review. Current Problems in Diagnostic Radiology. 2010; 39(4):160-85. [DOI:10.1067/j.cpradiol.2009.05.004]
Altay H, Kitis Ö, Çalli C, Yünten N. A spinal dermoid tumor that ruptured into the subarachnoidal space and syrinx cavity. Diagnostic and Interventional Radiology. 2006; 12(4):171-3. [PMID]
Patankar AP, Sheth JH. Dermoid cyst: A rare intramedullary inclusion cyst. Asian journal of neurosurgery. 2012; 7(2):81-3. [DOI:10.4103/1793-5482.98651] [PMID] [PMCID]
De Maio PN, Mikulis DJ, Kiehl TR, Guha A. AIRP best cases in radiologic-pathologic correlation: Spinal Conus dermoid cyst with lipid dissemination. Radiographics. 2012; 32(4):1215-21. [DOI:10.1148/rg.324115018] [PMID]
Calabrò F, Capellini C, Jinkins JR. Rupture of spinal dermoid tumors with spread of fatty droplets in the cerebrospinal fluid pathways. Neuroradiology. 2000; 42(8):572-9. [DOI:10.1007/s002340000345] [PMID]
Cha JG, Paik SH, Park JS, Park SJ, Kim DH, Lee HK. Ruptured spinal dermoid cyst with disseminated intracranial fat droplets. The British Journal of Radiology. 2006; 79(938):167-9. [DOI:10.1259/bjr/17232685] [PMID]
Winn HR. Youmans neurological surgery. Philadelphia: Elsevier; 2004.
Type of Study: Case report |
Subject:
Spine
Send email to the article author
| Rights and Permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
